Peer Reviewed
An Active-Duty Sailor With 2 Nonhealing Painless Ulcers: What’s Your Diagnosis?
Answer: Cutaneous Leishmaniasis
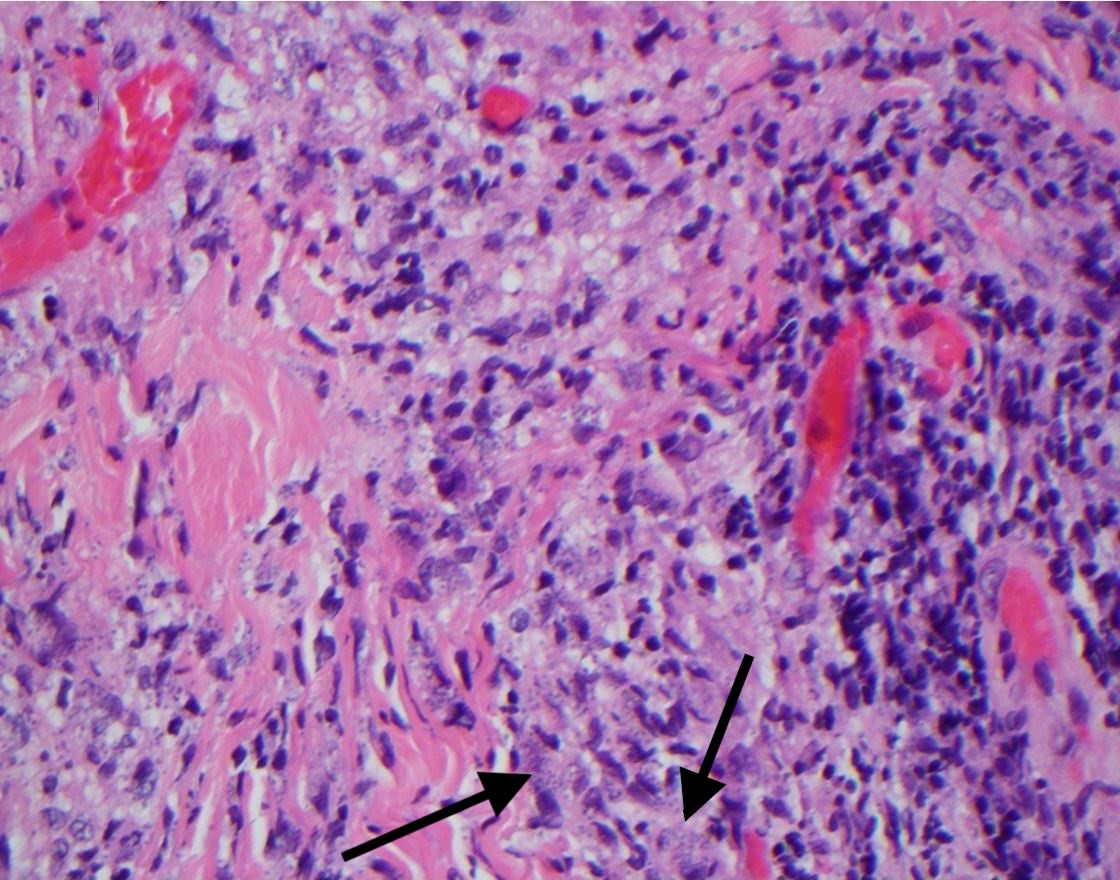
Results of a punch biopsy demonstrated multiple microorganisms (Leishmania amastigotes) within the dermal histiocytes (Figure 3) with negative acid-fast bacilli (AFB) staining results and negative cultures for aerobes, anaerobes, and fungi.

Figure 3. Histology results of a punch biopsy specimen showed Leishmania amastigotes in the dermal histiocytes (arrows).Discussion. Localized cutaneous leishmaniasis is a disease caused by the protozoan parasite Leishmania.1-3 The distribution is divided into Old World (Eastern Hemisphere, with the widest distribution in the Middle East, Mediterranean littoral, Arabian Peninsula, Africa, Indian subcontinent, and other areas)2,3 and New World (Western Hemisphere, typically in South America, Central America, and parts of Mexico)3 based on the distribution of species of Leishmania.
The typical clinical presentation is erythematous papules that enlarge and ulcerate, forming a broad-based, painless ulcer with or without crusting.2,3 These ulcers can mimic other infectious and noninfectious skin conditions. The disease is transmitted via bites of sand flies (Lutzomyia and Phlebotomus species), with a typical incubation period of weeks to months depending on the subtypes.2 In most cases, leishmaniasis lesions—also known as “oriental sores”—are self-limiting and heal spontaneously, taking months to years to resolve.2,3 The lesions often result in scarring that can be disfiguring, such when they affect the face or in cases of widespread distribution.2,4
Travel and exposure history are paramount to the diagnosis, with Iraq being a location of high prevalence of the disease and the sand fly vector.5 Leishmaniasis affects more than 1.2 million people worldwide3 and has a broad range of disease courses from limited cutaneous forms to diffuse mucocutaneous and visceral forms that can be fatal if left untreated.1,3
Differential Diagnosis >>
Differential diagnosis. Pustular syphilis, also known as malignant syphilis, is an atypical presentation of secondary syphilis. It is frequently associated with HIV coinfection and predisposing factors such as malnutrition, alcohol abuse, and debilitating illnesses.6 The rash typically presents as nodules and pustules, varying in size and widely distributed on the face, trunk, extremities, and/or genitals, and that ulcerate and often become necrotic.6 These ulcerated papules and nodules may be painful, and patients often present with other systemic symptoms such as fever, myalgia, arthralgia, or malaise.6 Histologic test results offer minimal benefit to diagnosis, because secondary cutaneous manifestations of syphilis vary, and findings of staining and direct visualization of spirochetes are often negative.7 Serologic evaluation is required for diagnosis. Given the reemergence of syphilis in recent years, secondary syphilis—“the great mimicker”—is always important to consider in the differential diagnosis.
Infection with Mycobacterium marinum, the most common atypical mycobacterium in humans, typically occurs following direct inoculation of the organism by abrasion or puncture in fresh or salt water.8,9 It typically presents as a violet-red papule or nodule that progresses to ulcer in persons with a history of exposure to nonchlorinated water within the past 2 to 3 weeks.8 The nodules spread in a sporotrichoid pattern (ie, lymphatic spreading of lesions) up the extensor surfaces of the affected extremity.8,9 A contributory occupational or social history, such as being an angler, swimmer, or aquarium worker,8,9 is common and distinguishes M marinum infection from Sporothrix infections seen in gardeners or landscapers. Histopathology findings of cutaneous mycobacterial infection typically consists of granulomas that range from poorly formed (loose infiltrates of epithelioid macrophages, scattered multinucleated giant cells, and lymphohistiocytic dermal inflammation) to well-formed granulomas (circumscribed, nodular macrophagic infiltrates).9 The granulomas can show central necrosis and suppuration with mixed inflammation and granulation tissue.9 AFB staining results are not always positive.9
Contact dermatitis is a localized inflammatory skin reaction to topical substances and is divided into irritant (direct cytotoxic effects) or allergic (T-cell mediated, hypersensitivity reaction).10,11 Benzoyl peroxide is a known irritant,10 and bacitracin is a common contact allergen.11 Lesions often present in mild to moderate cases as indurated, erythematous papules and plaques (with or without scale) that may itch or burn, with vesicles or bullae present in severe cases.11 Histopathology findings are similar to those of eczema, showing spongiosis (intracellular edema) in acute phases, but can progress to be acanthotic (epidermal hyperplasia) in cases of chronic exposure.7,10
Chromoblastomycosis is a chronic infection caused by traumatic inoculation of a number of fungal species, with high prevalence in Brazil, Mexico, Madagascar, the Dominican Republic, Venezuela, India, Japan, and Australia.12 The lesions commonly involve the lower extremities and present as painless papules that slowly progress over years to papillomatous or warty papules or plaques that are difficult to treat and may persist for decades.12 The lesions are typically misdiagnosed as cutaneous leishmaniasis, but on histology results show a lack of Leishmania amastigotes and a presence of thick-walled, brown, sclerotic bodies that are pathognomonic for the disease.12
Outcome of the case. The patient was referred to an infectious disease specialist. After a review of the most recent guidelines from the Infectious Diseases Society of America,4 he was treated with oral fluconazole, 200 mg daily, for 3 months, given the limited cutaneous involvement and better-tolerated side-effect profile of fluconazole. On follow-up, his papules had healed, leaving areas of pink scarring (Figures 4 and 5).
References:
- World Health Organization. Leishmaniasis: the disease and its epidemiology. http://www.who.int/leishmaniasis/disease_epidemiology/en/. Accessed July 24, 2018.
- Masmoudi A, Hariz W, Marrekchi S, Amouri M, Turki H. Old World cutaneous leishmaniasis: diagnosis and treatment. J Dermatol Case Rep. 2013;7(2):31-4
- Centers for Disease Control and Prevention. Parasites–leishmaniasis. https://www.cdc.gov/parasites/leishmaniasis/. Updated January 10, 201 Accessed July 24, 2018.
- Aronson N, Herwaldt BL, Libman M, et al. Diagnosis and treatment of leishmaniasis: clinical practice guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin Infect Dis. 2016;63(12):1539-1557.
- Coleman RE, Burkett DA, Putnam JL, et al. Impact of phlebotomine sand flies on U.S. Military operations at Tallil Air Base, Iraq: 1. background, military situation, and development of a “leishmaniasis control program.” J Med Entomol. 2006;43(4):647-662.
- Requena CB, Orasmo CR, Ocanha JP, Barraviera SRCS, Marques MEA, Marques SA. Malignant syphilis in an immunocompetent female patient. An Bras Dermatol. 2014;89(6):970-972.
- Rapini RP. Parasitic diseases. In: Rapini RP. Practical Dermatopathology. 2nd ed. Philadelphia, PA: Elsevier Saunders; 2012:219-230.
- Lata CJ, Edgar K, Vaughan S. Clinical implications for the timely diagnosis of Mycobacterium marinum in the age of biologic therapy: a case report and review of the literature. Case Rep Infect Dis. 2017;2017:5274302. doi:10.1155/2017/5274302
- Sia TY, Taimur S, Blau DM, et al. Clinical and pathological evaluation of Mycobacterium marinum group skin infections associated with fish markets in New York City. Clin Infect Dis. 2016;62(5):590-595.
- Cohen DE. Irritant contact dermatitis. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. Vol 1. 4th ed. Philadelphia, PA: Elsevier; 2017:262-274.
- Nixon RL, Mowad CM, Marks JG Jr. Allergic contact dermatitis. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. Vol 1. 4th ed. Philadelphia, PA: Elsevier; 2017:242-262.
- Verma S, Verma GK, Singh G, Kanga A, Sharma V, Gautam N. Facial chromoblastomycosis in sub-Himalayan region misdiagnosed as cutaneous leishmaniasis: brief report and review of Indian literature. Dermatol Online J. 2012;18(10):3.