
THE CASE: Child Protective Services (CPS) has asked you to evaluate a 6-month-old girl with a genital mass. The goal is to determine whether the "weird lump in the baby's private area"--noted while the child's diapers were being changed in day care--was the result of sexual abuse.
The baby's 18-year-old mother brings her to your office. The child is happy and in no distress. She interacts playfully with her mother and is developmentally appropriate. Her mother provides immunization records from the health department and from the urgent care clinic where she has taken her daughter for well-checks and for 2 visits for ear infections. The mother seems appropriately concerned and is able and willing to provide a detailed social history. She, her boyfriend (the baby's father), and the baby had all been staying with her mother (the maternal grandmother) since the patient's birth. The patient's father and grandmother did not get along well; he had moved out 3 weeks earlier, although he was still in contact with them. The mother had to return to work, and the baby had just started day care.
The mother admits that her boyfriend "has a temper," but he has never been violent or sexually aggressive. They have been dating for 3 years and have been "best friends" since childhood. The mother says she has never been sexually abused by her boyfriend and is unaware whether her boyfriend had been subject to sexual abuse. She doubts he would have ever done anything to harm their daughter.
The patient is well nourished (40th percentile for height, 60th percentile for weight). The skin is clear of bruises and marks. The baby moves all extremities with ease, and grabs for the stethoscope when being examined.
| Figure 1 - Image Not Available |
The genital examination is performed with the patient in her mother's lap. Gentle traction of the labia majora reveals a circumscribed mass lateral and superior to the right labia minora and clitoral hood (Figure 1). The mass is mildly compressible and rubbery. It is slightly warmer than the surrounding tissue. There is no edema surrounding the area. The remainder of the genitoanal exam is entirely normal.
You are not sure what this mass represents, but you have not seen it previously as a manifestation of sexual abuse. A call to the child abuse specialists in a nearby medical center confirms that such masses are not usually associated with abuse, and after some brainstorming, the possibility of a congenital vascular lesion comes up. You go back and question the mother who says that nothing like this was noted at birth. When the baby had a mild febrile illness at 2 months of age, however, the mother thought the area looked "different": she forgot to point this out at the clinic.
You obtain photos of the area and send them to a pediatric gynecologist. The physician thinks the mass is an infantile hemangioma and confirms this when the child is brought to her office for a visit. You agree to see the baby for monthly follow-up examinations.
The child's home environment is investigated, and a social worker refers the mother to appropriate agencies. Couples and family counseling is offered.
Over the next few months, the lesion grows slightly, but the child remains asymptomatic. The diagnosis of infantile hemangioma appears to be accurate. The child will be observed and photographs will be taken of the mass only at well-child checkups.
At the child's 2-year examination, the mass is no longer grossly visible and is barely palpable. At the 3-year examination, the lesion has resolved without sequelae.
DISCUSSION: GENITOANAL HEMANGIOMAS
Such lesions can be diagnostically challenging.1,2 They may be mistaken for child maltreatment because of their varied appearance and presentation.3 Incorrect diagnoses range from inflicted perineal burn injuries,3 to sexually transmitted infections, to sexual trauma.2
Congenital vascular anomalies, or "birthmarks" are common.1,3-5 It has been difficult to develop standardized nomenclature for these lesions because of their varied appearance.1,5 Traditionally, "hemangioma" has been used as a vaguely descriptive term for a wide variety of abnormalities.1,3,5 In 1996, the International Society for the Study of Vascular Anomalies adopted a classification system that groups birthmarks into 2 major groups (Table 1)1:
•Vascular tumors.
•Vascular malformations.
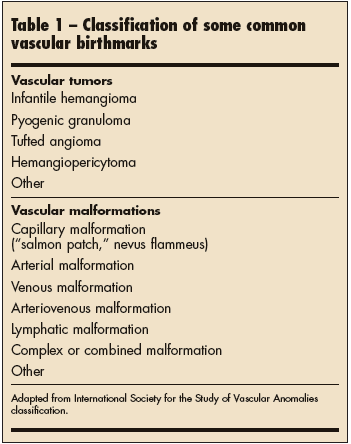
Further delineation is based on the lesion's clinical appearance and cellular features.1 The child in this case presented with the most common vascular tumor--the infantile hemangioma.1,3-5
Infantile hemangiomas affect up to 10% of all infants younger than 1 year.3 They are more common in Caucasians, females (female-to-male ratio, 3:1), and premature infants.1 Hemangiomas are now referred to as "superficial," "deep," or "mixed."1,4 Past terminology for superficial hemangiomas included "capillary" and "strawberry." Deep hemangiomas were referred to as "cavernous."1,4
Superficial hemangiomas are bright red or scarlet; they may be lobulated, plaque-like, or appear as lobulated papules, plaques, or nodules.1 They may partially blanch with pressure and are rubbery and noncompressible.1 Deep hemangiomas are subcutaneous, partially compressible, and often have an overlying blue hue, a prominent venous network, or telangiectasias.1 They can be warm to palpation.1 Mixed lesions have both superficial and deep components.1
A hemangioma can be present at birth or may first appear as a hypopigmented or hyperpigmented macule shortly thereafter.1,3-5 Typically, there is a period of rapid growth and expansion that lasts approximately 6 months. A plateau phase of several months is followed by an involution phase, which can take several years.1,3 Complications are rare. Ulceration occurs in 5%.3,4 Telangiectasias, scarring, atrophy, and fibro-fatty masses may persist after involution.1
Because infantile perineal hemangiomas exist in a warm, moist environment and are subjected to the repetitive trauma of wiping, they are at risk for ulceration.1,3,4 In fact, ulceration may be the presenting sign of a hemangioma if earlier subtle findings were missed.4 Ulcerations are often treated for an extended period as an infection before the correct diagnosis is made.4
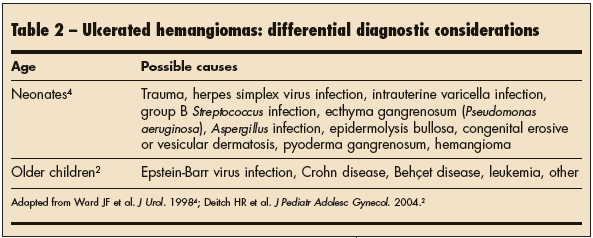
There is a broad differential diagnosis for ulcerated hemangiomas. A high-risk social history can lead to provider bias--with concern for sexually transmitted infection secondary to abuse at the top of the list.3 Ulcerations have also been mistaken for inflicted second and third degree burns, particularly in toddlers. Inflicted genitoanal burns in this age group almost always result from a caregiver's frustration surrounding toileting accidents.3 Other considerations in the differential are listed in Table 2.
Check for and record skin lesions and vascular birthmarks in children (Figures 2, 3, and 4). Serial photo documentation of these findings is an efficient and effective way to record their progression and clinical course.3 Photo documentation can be used to reassure parents during a slow involution; the images also provide an accessible record for other health care professionals.3 Patients and families will be saved time and trouble if a misdiagnosis later occurs.
| Figures 2, 3, and 4 - Images Not Available |
MANAGEMENT
Most infantile hemangiomas involute without intervention.1,3-5 Physicians should provide active non-intervention: this means inquiring about parental knowledge of the condition, offering education about the natural history and therapeutic options, and offering anticipatory guidance and support.1
Referral of a child with a perineal hemangioma to a pediatric gynecologist or urologist is never inappropriate. As noted, lesion ulceration can cause marked discomfort, functional compromise, and psychological stress.1,3-5
When treatment is necessary, options include topical corticosteroids, pulsed-dye laser therapy, and (rarely) surgical excision.1,4,5 Ulcerated lesions should be treated with topical or oral antibiotics, local wound care/dressing, and adequate pain control.1,4 Pulsed-dye laser therapy shortens the time to resolution and has been quite effective.1,4
Other treatments include interferon alpha-2a or -2b or vincristine.1 These medications are reserved for lesions that are resistant to other treatments and that threaten life or function.
In short, perineal hemangiomas are diagnostically challenging entities for the primary care provider. These lesions can be easily mistaken for evidence of sexual trauma or physical abuse. Serial photographic documentation and careful logging of physical findings can help track the clinical course and avoid causing unnecessary psychosocial stress to families associated with investigations that are based on inaccurate diagnoses.