
Agoraphobia: When an Older Woman Refuses to Leave Home
Case Presentation
Ms. M is a 45-year-old divorced woman who makes an appointment for her 78-year-old mother with a psychiatrist. On the day of the appointment, Ms. M arrives alone, asking to meet with the psychiatrist. Ms. M appears distressed and worried. She explains that her mother, Mrs. S, has not left her apartment in the past four years. Ms. M has arranged for food to be delivered and has hired a housekeeper who performs cleaning and laundry tasks. She has tried numerous times to take her mother out, but Mrs. S refuses.
Ms. M describes her mother as an “anxious person” who always had difficulty going places far from their apartment. She reports that the severity of her current problem became apparent when Mrs. S refused to travel to another state to visit her first grandchild six years ago. Mrs. S has stopped seeing doctors and, while she talks to friends and family on the telephone, has almost no visitors. Ms. M reports that her mother appears calm but refuses to even discuss going outside. She calls her mother during the session and asks permission to discuss her problem with the psychiatrist. Mrs. S is polite and agrees to have her daughter provide her entire history. Mrs. S also adds that she plans on staying home and thanks both her daughter and the psychiatrist for their concern.
Ms. M is eager to provide history, even when counseled that she may need to focus more on her own life. Ms. M tells the psychiatrist that her mother is a widow who has three grown children. Following the death of her husband seven years ago, Mrs. S started staying inside her apartment for increasing periods of time. Ms. M reports that as a child she would often see her mother hyperventilate and appear very nervous when they attended family gatherings. She describes her father as a very demanding person who would simply insist that her mother go out, even carrying her down the stairs if she refused to leave.
Ms. M denies seeing any physical abuse but remembers that her mother often became acutely distressed, with periods of hyperventilating and complaining that she was unable to breathe. She and her sister often accompanied their mother to the family doctor, who told them that it was “nerves.” Ms. M reports that her mother never had any psychiatric evaluation or treatment, but she knows that she clearly has some type of anxiety or panic disorder. Ms. M asks the psychiatrist to prescribe some medication that will help her mother, and she becomes angry when told that her mother must be evaluated in person and undergo at least some basic medical tests. Ms. M leaves the office, telling the psychiatrist that the session was just a waste of time.
Discussion
Agoraphobia is a clinical term that refers to a persistent and pathologic fear of public places.1 Patients with agoraphobia frequently also have panic disorder and develop agoraphobia in response to the panic attacks that occur suddenly and spontaneously, causing significant anticipatory anxiety. In the later stages of the illness, patients will stay at home rather than risk having panic symptoms when outside.1,2 Agoraphobia is a disorder that is included in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, text revision (DSM-IV-TR) as part of the panic disorder spectrum and is diagnosed as occurring with or without overt panic attacks.1
The ability to recognize and effectively treat anxiety in older adults is important, given the debilitating effects that an unhealthy level of anxiety can have in this vulnerable population.2,3 Panic disorder and agoraphobia are chronic illnesses that often have been present for decades.3 Agoraphobia is twice as common among women as compared to men.2 It commonly has an onset in early adulthood but is typically a chronic illness characterized by exacerbations and remissions.1-3 Traumatic events can lead to relapses and cause severe episodes, such as the complete refusal to leave one’s residence.1,2,5
Panic disorder is characterized by chronic, repeated, and unexpected panic attacks, bouts of overwhelming and irrational fear, terror, or dread without any specific identifiable cause.1 During a panic attack, the person experiences a constellation of physical and cognitive symptoms that can include palpitations, sweating, trembling, shortness of breath, the feeling of choking, chest pain or discomfort, nausea or abdominal distress, dizziness or lightheadedness, feelings of derealization or depersonalization, paresthesias, chills or hot flashes, fear of losing control, “going crazy,” or dying.1,2 A diagnosis of a true panic attack requires that at least four of the somatic symptoms listed above are experienced.1 Attacks are brief, lasting typically 10-30 minutes, but may seem much longer to the suffering patient.
In between panic attacks, individuals with panic disorder worry excessively about when and where the next attack may occur.4,5 A clinically significant degree of panic symptoms exists if the history reveals that recurrent and unpredictable panic attacks have occurred for at least 1 month and that time is being spent in worried anticipation of possible recurrence.1,2 Whether agoraphobia related to the panic attacks is present also needs to be considered. In such cases, agoraphobia involves the persistent fear of situations that can trigger a panic attack, such as when a patient reports remaining at home to avoid an attack. Patients who experience one or more panic attacks may not necessarily warrant a diagnosis of panic disorder. Panic attacks in late life often present with limited symptoms often related to one or two organ systems, such as shortness of breath, nausea and diarrhea, overwhelming feelings of pounding in the chest, or dizziness.2 These limited-symptom panic attacks are accompanied by feelings of doom, dread, or fears of dying.
Other phobias less severe than agoraphobia include specific phobia, simple phobia, and social phobia. A specific phobia is defined as a marked, persistent, excessive, unreasonable fear in the presence of or in anticipation of a particular distinct trigger, such as a specific person, animal, place, object, event, or situation.1,2 Commonly, the patient’s anxiety level increases instantly when the feared trigger is encountered. Interestingly, he or she is able to identify this fear as unrealistic and unsupported, even though the cognitive and physiologic responses persist.5-7 Specific phobias often involve a great amount of anticipatory anxiety, such as thoughts of just the possibility of encountering the feared stimulus, and avoidance behaviors are likely to be reported. The consequence is that the person experiences a variety of personal difficulties as a result of the anxiety. These behaviors interfere with work and daily routines, and they decrease the person’s opportunities to experience pleasurable situations due to fear that a trigger might be present.2-4 They can also contribute to secondary symptoms, such as frustration, hopelessness, and a sense of lack of control in one’s life.7
Examples of simple phobias include fear of mice, dogs, elevators, flying, or heights. Frequently, specific phobias are seen with panic disorder, with or without agoraphobia.2 Among older adults, especially in urban settings, fear of crime seems to be particularly prevalent. Phobic disorders tend to be chronic and persist into old age. However, fear of falling is a specific phobia that is increasingly recognized to have an onset in later life.4
Patients with social phobia have fears that they will behave in a manner that is inept or embarrassing while in a public place or setting.1 Commonly, the fear is that of trembling, blushing, or sweating profusely in social situations.3,4 Other common fears involve speaking in public, going out to a restaurant, or simply socializing with others at a function or party. Similar to specific phobias, social phobia is often accompanied by a significant degree of anticipatory anxiety or avoidance.1,3 Although systematic studies of social phobia in older adults are lacking, epidemiologic data indicate that this disorder is chronic and persistent in old age. Common manifestations in old age include the inability to eat food in the presence of strangers, and—especially in men—being unable to urinate in public lavatories.4,5
Assessment of anxiety in older adults generally begins with a clinical psychiatric interview to determine the course and nature of symptoms. The interview should include an evaluation of the patient’s mental status, including appearance, mood, and behavior.1,2 Consideration of the patient’s social situation and support systems is particularly relevant in the geriatric population. Assessment of any impairment in functional status related to the anxiety is an important part of the evaluation. A review of all medications, including prescription, over-the-counter, and herbal supplements, should be done to exclude a medical or pharmacologic cause for what appears to be an anxiety disorder, or to identify an aggravating condition. Laboratory tests to check for common medical conditions such as renal, thyroid, or hematologic diseases are important. Urine toxicology should be considered in cases in which substance abuse or misuse is suspected.1-3
It is common to encounter older patients with comorbid anxiety and medical disorders. In many cases, medical illness can mimic an anxiety disorder in its presentation. Medical illness can also exacerbate a concurrent anxiety disorder. Finally, adverse events of medications can produce or contribute to anxiety symptoms. Common medical illnesses that can cause or contribute to an anxiety disorder include cardiovascular or pulmonary conditions and hyperthyroidism.1,2 Common medical conditions that can be exacerbated by high levels of anxiety include angina pectoris, myocardial infarction, gastroesophageal reflux disease, chronic obstructive pulmonary disease, and hypertension.4
Antidepressants have proved efficacious in the treatment of panic disorder. Studies have demonstrated that selective serotonin reuptake inhibitors (SSRIs) are safe and efficacious in the specific treatment of late-life anxiety disorders.3,6 Given their relatively favorable adverse-event profile, the SSRIs or serotonin-norepinephrine reuptake inhibitors (SNRIs) should now be considered the medications of choice for these disorders. Further, SSRIs should also be considered agents of choice for treating depression with severe anxiety symptoms.4,6,7 Compounds such as the SNRIs venlafaxine and duloxetine should be considered as alternatives for those patients who do not respond to SSRIs or who develop adverse events2,4,6-9 (Table).
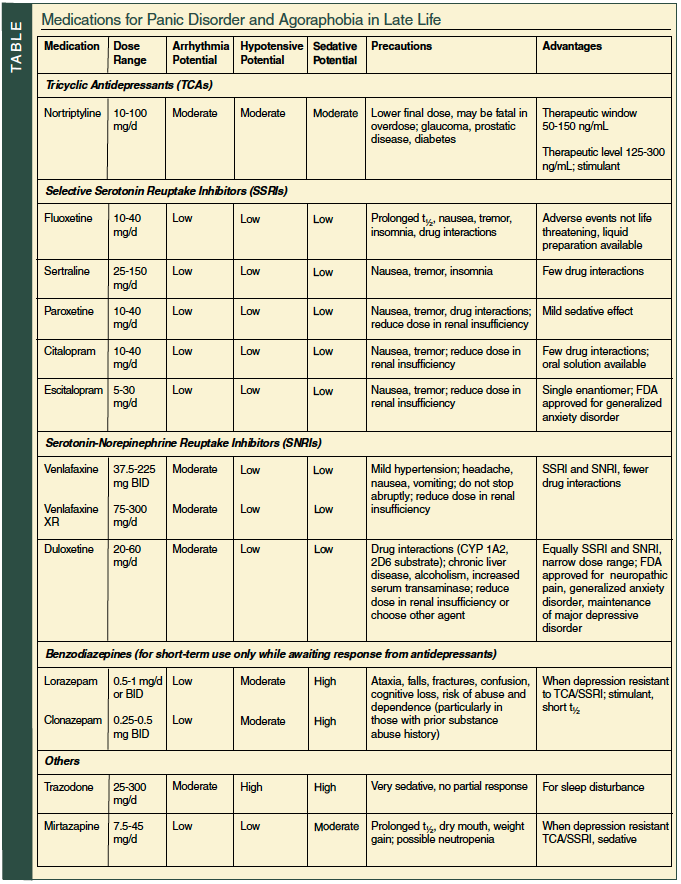
Over the past several decades, benzodiazepines have been the most commonly prescribed anxiolytics for both younger and older patients, but their use is now discouraged as first-line therapy.8,9 If symptoms are severe, benzodiazepines with shorter half-lives or without active metabolites, such as lorazepam and clonazepam, are preferable in treating older adults because they are metabolized by direct conjugation, a process relatively unaffected by aging. However, the use of even short-acting benzodiazepines should be limited to 6 months or less because long-term use is associated with multiple complications, such as motor incoordination and falls, cognitive impairment, depression, and the potential for abuse and dependence.2,8,9
Although antihistamines such as hydroxyzine and diphenhydramine are sometimes used to manage mild anxiety in younger patients, the anticholinergic properties of these agents can cause serious problems in older adults, and their use is not recommended.2,5 Antipsychotic medications such as risperidone, olanzapine, quetiapine, and haloperidol are not considered appropriate choices for treatment of a nonpsychotic older adult with an anxiety disorder.2
Although pharmacotherapy is commonly the first-line treatment for late-life anxiety disorders, psychological and behavioral treatments are often efficacious, either alone or as adjuncts to medication.3,5-7 The psychotherapeutic remedies that have been most rigorously tested all fall under the rubric of cognitive-behavioral therapy.3,7,8 Techniques generally fall into three categories: (1) relaxation training used with music, visual imagery, aromatherapy, and instruction in relaxation techniques; (2) cognitive restructuring to help the patient identify triggers and stimuli that maintain anxiety, gain more control over the effect of such stimuli, and develop a range of coping strategies and tools; and (3) exposure with response prevention, in which the individual is gradually exposed to the feared stimuli. Graded desensitization, which is used in panic symptoms and phobias, relies on exposure to gradually more anxiety-producing stimuli, with techniques to manage and tolerate the resultant anxiety. Treatment of older adults typically includes a combination of these therapeutic approaches.3-7
The clinician must be mindful of the cultural differences in the presentation of panic and anxiety symptoms. For example, in many Asian cultures, anxiety is often expressed through somatic complaints including headaches, back pain, chest tightness, shortness of breath, fatigue, dizziness, and gastrointestinal complaints. Patients may be very reluctant to discuss any emotional or psychological component to these symptoms. In many Latin-American patients, the experience of anxiety is expressed as agitation, weakness, fainting, and cardiac symptoms.1,2 It is important to validate the symptoms and explore the treatment options with the patient that will focus on the alleviation of distress.
Information about anxiety disorders for patients and family members may be downloaded from the National Institute of Mental Health website at www.nimh.nih.gov and the Anxiety Disorders Association of America website at www.adaa.org.
Outcome of the Case Patient
The case of Mrs. S was complicated by her unwillingness to accept treatment. Her daughter was referred to a local support group for patients with anxiety disorders and their family members, but she did not want to attend. Ms. M was also offered referrals to private case management services that offer home visits, and she hired a private social worker to see her mother. Mrs. S allowed the social worker to visit her in her apartment and met with her several times. She continued to refuse any option of leaving her apartment and refused the services of a visiting doctors program. After six months, Mrs. S remained homebound by choice but was accepting some home services and continued to see her social worker. Her daughter remained frustrated by her mother’s behavior but felt better knowing that more services were in place.
The author reports no relevant financial relationships.
Dr. Lantz is Chief of Geriatric Psychiatry, Beth Israel Medical Center, First Ave @ 16th Street #6K40, New York, NY 10003; (212) 420-2457; fax: (212) 844-7659; e-mail: mlantz@chpnet.org.