
Bilateral Flank Pain in an Older Adult
An obese 65-year-old man presented to the emergency department with a 1-day history of bilateral flank pain, which was greater on his right side than his left. Four days earlier, he had diarrhea accompanied by fever and chills, which lasted for one day. The patient reported no vomiting, constipation, dysuria, hematuria, or bright red blood in his stools. His medical history was significant for insulin-dependent diabetes mellitus and hypertension. His surgical history included an appendectomy and a prostatectomy for carcinoma. The patient’s medications included insulin, metformin, and nifedipine. Although the patient was a current smoker, he denied illicit drug use or chronic alcohol consumption.
During the physical examination, the patient was in no distress. His vital signs included a heart rate of 99 beats per minute, temperature of 97.8°F, blood pressure of 133/68 mm Hg, and a respiratory rate of 16 breaths per minute. His abdomen was tender to palpation in the right upper and right lower quadrants, without guarding or rebound. The remainder of the physical examination was unremarkable. Urinalysis revealed trace ketones, but all other laboratory values were within normal limits.
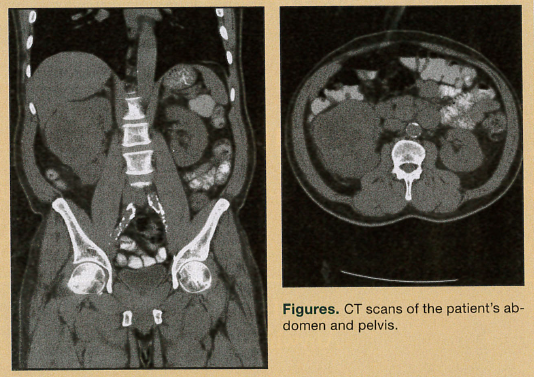
Abdominal radiographs revealed multiple loops of bowel with air-fluid levels, but no definite obstruction. Computed tomography (CT) scans of his abdomen and pelvis were performed (Figures).
Based on the case description and the CT scans above, what is your diagnosis?
A. Right renal simple cyst
B. Mass at the head of the pancreas
C. Perinephric hematoma
D. Renal cell carcinoma
E. Right renal abscess
Answer and Discussion on next page
Diagnosis: Renal cell carcinoma (D)
Discussion
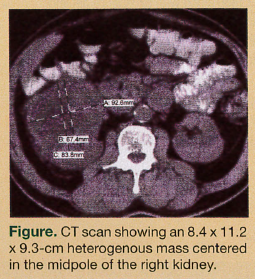 The patient has renal cell carcinoma (RCC), which is the most common primary malignancy of the kidneys. Patients with these tumors may present with flank pain, hematuria, erythrocytosis, or a combination of these findings. The case patient’s CT scan shows a heterogenous mass, measuring 8.4 cm by 11.2 cm by 9.3 cm, centered in the midpole of the right kidney (Figure). Perinephric stranding and multiple pericaval lymph nodes measuring up to 8 mm are also visible.
The patient has renal cell carcinoma (RCC), which is the most common primary malignancy of the kidneys. Patients with these tumors may present with flank pain, hematuria, erythrocytosis, or a combination of these findings. The case patient’s CT scan shows a heterogenous mass, measuring 8.4 cm by 11.2 cm by 9.3 cm, centered in the midpole of the right kidney (Figure). Perinephric stranding and multiple pericaval lymph nodes measuring up to 8 mm are also visible.
Currently, most RCC cases (70%) are found incidentally and are small early-stage lesions.1-3 When found early, generally before symptoms manifest, these lesions are amenable to limited renal resection, which is nephron-sparing. Studies have shown that lesions in symptomatic patients tend to be larger and have a more aggressive histology, leading to a poorer prognosis.3 One study reported that tumors larger than 5 cm are likely to cause symptoms.1,4 If the tumor is confined to the kidneys, the 5-year survival rate after nephrectomy is 60% to 90%, which drops to between 5% and 10% in individuals with distant metastases. Spindle cell and anaplastic lesions are more aggressive and have a worse prognosis than clear cell tumors. The presence of regional lymph node metastases also signifies a poor prognosis.1
Kidney masses include RCC (about 98% of malignant tumors), lymphoma, oncocytoma (the most common benign solid kidney tumor), angiomyolipomas, and metastatic disease.5 Accurate imaging assists in determining the type and stage of the renal lesion. This is important for treatment planning, as it enables surgeons to determine whether partial nephrectomy will be curative. Imaging can reveal the extent of tumor invasion into the renal sinus fat, renal vein, and renal collecting system. Evidence of lymphadenopathy and morphology of the contralateral kidney is also demonstrated. Recent advances in radiological techniques with multidetector spiral CT scanning with triphasic imaging has proven beneficial to characterize and stage lesions. Magnetic resonance imaging (MRI) is also a valuable tool. MRI can be used in patients with allergies to iodinated contrast medium and those with renal insufficiency. MRI can also show patency of blood vessels without use of intravenous contrast medium.5,6
Examining the Other Answers
The other options for this quiz included right renal simple cyst, mass at the head of the pancreas, perinephric hematoma, and renal abscess.
Right Renal Simple Cyst. Renal cysts are the most common renal space-occupying lesion. About 50% of people over the age of 50 years have one or more renal cysts. Of these lesions, 80% are simple cysts and most are asymptomatic. On ultrasonography, they appear as anechoic lesions with very well-defined back walls.5
Mass at the Head of the Pancreas. Of pancreatic cancers, 60% develop in the pancreatic head. Patients with these lesions commonly present with epigastric abdominal pain, weight loss, and jaundice. CT scans will show the primary tumor, local invasiveness, lymph node involvement, presence of metastatic liver masses, and extent of peritoneal spread. MRI with gadolinium enhancement may differentiate cancer from chronic pancreatitis and help clinicians assess the pancreatic and bile ducts.7
Perinephric Hematoma. Hematomas are usually associated with trauma. On CT scanning, perinephric hematomas may have a mass-like appearance and be surrounded by fat stranding. Chronic hematomas may also show calcifications.5
Renal Abscess. Patients with a renal abscess usually present with fever. Other common findings include leukocytosis and elevated sedimentation rate. On CT scanning, renal abscess appears as a nonlobar, homogenous, low-density intrarenal lesion.8
The authors report no relevant financial relationships.
References
1. Sheth S, Scatarige J, Horton KM, Corl FM, Fishman EK. Current concepts in the diagnosis and management of renal cell carcinoma: role of multidetector CT and three-dimensional CT. Radiographics. 2001;21:S237-S254.
2. Lee CT, Katz J, Fearn PA, Russo P. Mode of presentation of renal cell carcinoma provides prognostic information. Urol Oncol. 2002;7(4):135-140.
3. Chen DY, Uzzo RG. Evaluation and management of the renal mass. Med Clin North Am. 2011;95(1): 179-189.
4. Schips L, Lipsky K, Zigeuner R, et al. Impact of tumor-associated symptoms on the prognosis of patients with renal cell carcinoma: a single-center experience of 683 patients. Urology. 2003;62(6):1024-1028.
5. Marhuenda A, Martín MI, Deltoro C, Santos J, Rubio Briones J. Radiological evaluation of small renal masses (I): pretreatment management. Adv in Urology. 2008:415848.
6. Walter C, Kruessell M, Gindele A, Brochhagen HG, Grossmann A, Landwehr P. Imaging of renal lesions: evaluation of fast MRI and helical CT. Br J Radiol. 2003;76(910):699-703.
7. Conwell DL. Pancreatic Neoplasm. Cleveland Clinic Foundation. www.clevelandclinicmeded.com/medicalpubs/.../pancreatic-neoplasm. Accessed March 12, 2012.
8. Cronan JJ, Amis ES Jr, Dorfman GS. Percutaneous drainage of renal abscesses. AJR Am J Roentgenol. 1984;142(2):351-354.