
Case Controversies in Genetic Medicine: Women With Breast Cancer
ABSTRACT: After recent publicity surrounding actress Angelina Jolie’s choices regarding preventive surgery, this roundtable discussion features a medical geneticist (Dr Wilson), a breast surgeon (Dr Rahman) and an internist (Dr Kaplan) to address current options for breast-ovarian cancer testing and management. The discussion considers new advances in genetic medicine, their relevance to primary care physicians, and the roles of generalists vs. subspecialists in recognizing, testing, and counseling for genetic susceptibility.
______________________________________________________________________________________________________________________________
How are the terms “personalized medicine” and “DNA/protein profiling” relevant to primary care?
GW, Genetics: DNA isolation, expression, and rapid sequencing technologies have provided molecular markers1-3 that extend laboratory tests from their traditional roles in differential diagnosis to those of disease predictions (presymptomatic diagnoses) or drug effects (pharmacogenetics).4 The most surprising finding of human genomic medicine—now able to sequence individual genomes in a few days using NextGen or massive parallel sequencing—has been the extraordinary extent of variation: Humans have sequence differences every 3-400 nucleotides totaling up to 10 million differences in our 3 billion nucleotide genome.1-5 These are mostly benign variants, either single nucleotide polymorphisms (SNPs) detected by DNA sequencing or extra/missing DNA segments known as copy number variants (CNVs) detected by high resolution chromosome (microarray) analysis.1
Because these DNA variations will be passed down in families and cluster in geographic (ethnic) groups, they can serve as markers for nearby genes that transmit the hereditary component of (genetic predisposition to) disease. DNA markers can modify risks for multifactorial disorders like autism, diabetes, coronary artery disease, schizophrenia, and later-onset cancers by forecasting genetic susceptibilities complementing environmental factors) that cause disease.2, 3
The large number of human gene variants ensures that one or more will be near disease-causing loci, available to modify individual disease risk. This approach is analogous to the use of HLA variants to predict risk for diseases like hemochromatosis (OMIM235200).5 The hemochromatosis HFE gene lies near the HLA cluster on chromosome 6 and thus travels with it in families, showing linkage disequilibrium or allele association.2,3 Other associated alleles, such as HLA B27 that is more common in individuals with ankylosing spondylitis (OMIM106300), may participate in the disease process as postulated for apoE variants and Alzheimer disease (OMIM104300). Whether by disease mutation (DNA diagnosis), DNA marker (risk modification), or examination of multiple DNA/protein species (molecular profiling, array analysis), genetic testing is increasingly promoted by commercial companies or academic for-profit laboratories. These laboratories often advertise to physicians and patients (direct-to-consumer testing), and are highlighted in lay medical and news media.6
As a subspecialist who also does general pediatrics, I recognize the extraordinary range of medical knowledge that primary care practice must encompass and the scheduling/economic challenges in conveying technical information to patients. At the same time, I feel that practitioner experience and judgment acquired from the use of traditional markers, such as prostate-specific antigen tests or lipid profiles, is critical for guiding patients who consider genetic testing and gene profiling.7
RR, Surgery: The importance of genetic profiling for a breast surgical oncologist has two aspects: (i) the patient’s personal genetic risk that will guide cancer prevention and/or treatment planning, and (ii) the tumor genetic profile that may predict prognosis and response to therapy.8-11 For the patient’s personal genetic profile, it is important to know if the presenting cancer is hereditary in nature. Strong family history, young age at first cancer, and bilaterality all are clues that the cancer is hereditary.10 Hereditary cancers have higher recurrence rates and chances for contralateral cancer, key factors for the patient deciding whether to have local surgery versus bilateral mastectomy.
Knowledge of the presence of a hereditary mutation becomes important since BRCA I or II genetic mutations confer cancer risks as high as 85% for breast and 44% for ovarian cancer.9 Although bilateral mastectomy and oophorectomy are aggressive and invasive steps, they have significant success in preventing cancer and tilt the risk-benefit ratio heavily in favor of surgery.8-10 As a breast surgical oncologist, I recommend that women with BRCA1 or 2 mutations plan prophylactic mastectomy and oophorectomy. Of course, the issues around completion of family, body image, and options of reconstruction have to be worked out during counseling sessions.
The second area of importance for the surgical specialist is tumor genetics, where gene content and expression of the breast tumor are profiled.10 We now know that breast cancers with certain genetic profiles are more aggressive than others and more responsive to specific therapeutic agents. Contemporary practice dictates that certain tumors including breast cancers undergo gene content and expression profiling to guide prognosis and treatment options.
LK, Primary Care Practice: One of the key challenges in primary care is the ability to recognize both the strengths and weaknesses in your fund of knowledge as a physician, and to provide clinical care only within that range. Despite the evidence that the vast majority of diagnoses are made based upon a medical history,6 there is still question as to the validity of the information collected.7 Although all physicians studied genetics in medical school, it is only in the past 10 years that the practical application of this has filtered to clinical practice, with the term “personalized medicine” coming in vogue.12 As with all physicians, it is incumbent on primary care physicians to stay “current” with the medical literature; the use of genetic testing is only one component of that. How this information and technology is ultimately applied to clinical practice in a cost-effective manner13 will be an ongoing issue.
What can you tell us about pedigree sketches, genetic screening/testing, and the guidelines for primary care practitioners? Use the two cases described below.
Case 1. Lois, a 58-year-old African-American woman, developed a unilateral breast lump that was biopsied and found to contain adenocarcinoma. Lois has a 45-year-old sister, a 47-year-old brother, and two daughters (age 22 and 19) who are healthy. Her mother, Lola, is in her 70s and is healthy aside from diabetes; her father died at 69 of myocardial infarction.
Case 2. Barbara, a 30-year-old Ashkenazi Jewish woman, recently received a diagnosis of breast cancer after a routine mammography that showed bilateral suspicious lesions. Barbara initiated the annual screening in her late 20s because her mother, Janice, developed breast cancer at 33 and died of the disease at 35. Family history reveals that Barbara has 31-year-old identical twin sisters, Edith and Edna and a 29-year-old brother, Edward. Barbara has a teenage son and daughter, and Edith has an 8-year-old daughter. Barbara’s mother has three sisters including Gretchen, who developed ovarian cancer at 37, and a brother, Ethan, who died of prostate cancer at 39. Ethan had two daughters and Gretchen has one daughter and one son—all in their 20s.
GW, Genetics: An informative family history is rare even in a genetics clinic, and I feel that standard family history questionnaires are adequate for screening in a general practice. A pedigree sketch (Figure 1) is required only when several individuals in a family have the same or similar diseases as exemplified by the above example of Case 2, but here sketches are provided for both cases to illustrate common symbols—circles for females, squares for males, generations aligned, filled symbols for individuals with similar diseases, slashes for death, and an arrow pointing to the individual that prompted concern (proband or consultand that roots the pedigree).
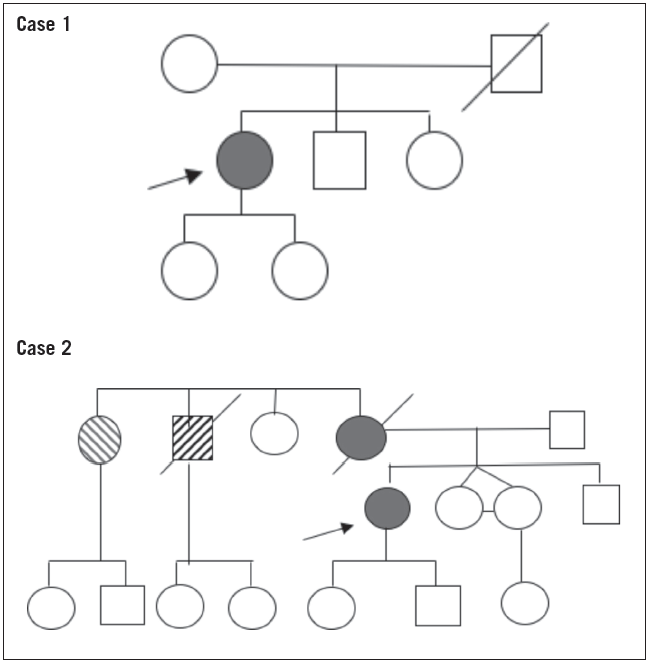
Figure 1. Pedigree sketches for cases 1 and 2.
The older woman in Case 1 has no family history of breast cancer, suggesting that her cancer reflects multifactorial determination (interaction of several genes and environmental factors) that causes most later-onset cancers. As DNA markers become better characterized and more informative, such women may have DNA profiling to define the degree of hereditary risk and that for their children in the way a patient with ankylosing spondylitis might have HLA B27 testing to define a hereditary factor for their arthritis that can be examined in their children. Women with a DNA marker associated with later-onset breast cancer, like a patient having a HLA B27 allele, would have a defined hereditary factor in their cancer that could be examined in their children. Children testing positive for the DNA marker (or HLA B27) would know they had increased susceptibility for the cancer (spondylitis), their risks higher than those with a negative test but only conveying increased risk rather than a certain diagnosis. As DNA markers become better characterized and their associated disease risks better defined, three-generation family histories for common disorders like diabetes or schizophrenia may become as routine as those now performed for Mendelian disorders like cystic fibrosis or sickle cell anemia.
The situation in Case 2 is very different, for this woman is younger and has a positive family history that suggests autosomal dominant inheritance (males and females in two generations are affected provided that one recognizes variable expression as ovarian, breast, or prostate cancer). Autosomal dominant inheritance implies that a single gene determines risk and mandates that options for breast-ovarian cancer gene testing (BRCA1—OMIM604370 and BRCA2--OMIM612555) be offered. DNA testing for BRCA mutations can now be performed with high sensitivity,14,15 and a recent Supreme Court decision nullifying patenting of particular genes (but not of gene testing methods) should broaden testing options and decrease prices (now in the range of $3500). BRCA1 and 2 mutations are estimated to account for about 10% of breast cancer cases overall, with higher numbers for young women or those of Ashkenazi Jewish origin as with Case 2.
Affected family members in Case 2 would have one normal and one abnormal BRCA allele, giving each of their offspring a 50% risk of receiving the abnormal BRCA mutation with is associated high risks for breast/ovarian cancer that prompts consideration of mastectomy/oophorectomy as discussed by Dr. Rahman above. The woman in Case 1 would confer multifactorial risks for breast cancer (and no higher risks for ovarian cancer) to her offspring, averaging about 5% when a parent has a disorder like diabetes mellitus or a birth defect like cleft palate. The slight increase in risk could be further modified if DNA markers for multifactorial breast cancer were available, increasing risk slightly if offspring inherited the marker, lowering it if they did not. Even without DNA markers, extensive experience with breast cancer allows these multifactorial risks to be estimated using in statistical models as discussed by Dr. Rahman.
RR, Surgery: For patients who decide against prophylactic surgery (in the case of genetic mutation) or for patients who have significant risk factors but do not have known genetic mutations, a high-risk screening and prevention strategy is the best approach. Several mathematical models, based on reproductive history and other factors, have been shown to predict a woman’s risk of developing breast cancer over her lifetime.
The Gail model is most frequently used in the United States.16 It is very easy to use but tends to underestimate the risk of breast cancer. It is a little unnerving in that it does not take into account non-first degree relatives with breast cancer.
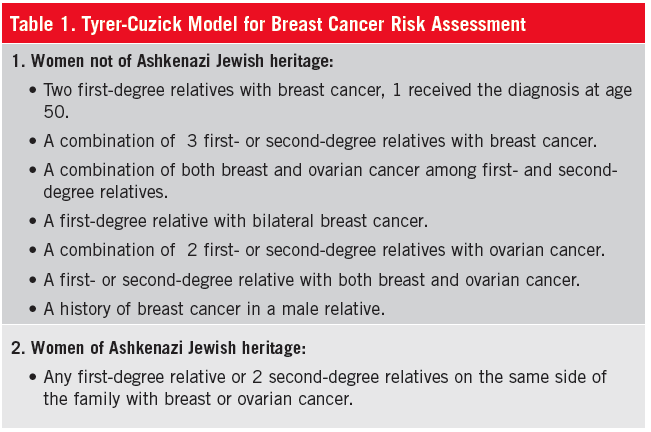
I use the Tyrer-Cuzick model, which has shown to be more accurate through several studies, for risk calculation (Table).16 This European model takes into account many more factors than the Gail model, calculating the risk of carrying a genetic mutation in addition to the risk of breast cancer. Once a 5% risk over a decade is predicted,16 women should be counseled regarding lifestyle changes
—e.g., maintaining ideal body weight, regular exercise program, minimizing alcohol intake, cessation of smoking—and the possibility of chemoprevention with tamoxifen or raloxifene. Whereas 5% is a significant risk, it is not high enough to justify prophylactic surgery. These women should be enrolled in a high-risk screening program for breast examination and mammographic screening at 6-month intervals. Women with a lifetime risk >20% may need an MRI screening in addition to mammograms.8-10, 16
LK, Primary Care Practice: Suggested guidelines for screening of common diseases that involve genetic testing are published on an ongoing basis by the US Preventive Services Task Force,17 a division of the Agency for Healthcare Research and Quality/US Department of Health and Human Services. It is imperative that primary care physicians be involved in these decisions, although UK surveys suggest that most primary care physicians do not feel adequately prepared to do so.18
How would these genetic testing change medical management and preventive health care?
GW, Genetics: The presence of BRCA1 or BRCA2 mutations confers significant lifetime risks for breast or ovarian cancer (Figure 2). The testing relies on sequencing of the BRCA genes in at-risk individuals and is highly accurate. False-positives (sequence variations that are benign polymorphisms) or false-negatives (normal BRCA1/BRCA2 sequencing that misses other cancer gene mutations) are less common for breast cancer testing than for other genetic cancers (eg, Lynch—OMIM120435, Gardner—OMIM175100, Gorlin—OMIM109400, or Li-Fraumeni—
151623 syndromes).

Figure 2. Breast and ovarian cancer risks in BRCA mutation carriers vs. the general population (Courtesy: Myriad Genetics).
LK, Primary Care Practice: Medical care clearly evolves over time. Twenty years ago, routine colorectal cancer screening involved serial fecal occult blood cards and intermittent flexible sigmoidoscopy. Today the gold standard is a colonoscopy.19 Recent controversy over mammography screening has brought into light the notions of “sensitivity” and “predictive value” in testing, as well as the implications of organizations that have different guidelines20 and their public interpretation.
As a primary care physician, the most significant benefit is the ability to help my patients interpret these conflicting opinions in the context of their own health.21 Generalists, by their very nature, must be able to evaluate patient-based information and screening recommendations in light of their patient’s overall health. Screening must be tailored to a particular patient, rather than targeted to the particular demographic group in which the patient resides.
What economic and ethical considerations apply to genetic testing?
GW, Genetics: Initial testing for BRCA1 and BRCA2 mutations costs around $3,500 and is covered by most insurance plans.15 The former monopoly on BRCA testing by one company meant that self-pay or Medicaid patients had to negotiate costs of about $1,000 self-pay with installments being possible.22, 23 These costs are not out of line with those for other gene (DNA) tests, averaging around $1,000 to $3,000 per test and available for over 1,000 genetic diseases.14 The new exome sequencing test examines the coding regions of all 23,000 human genes for around $9,000, bringing hopes for less expensive testing when it is better characterized and more routine.1 However, the ability to test all genes by exome sequencing brings another complication besides distinguishing normal variation from true mutation: the possibility of incidental findings. Exome sequencing for a concern like mental disability might find a mutation in BRCA 1 or 2, mandating that patient preferences to know or not know incidental DNA findings be documented during consent.
At present, DNA testing is affordable only for common disorders like cystic fibrosis or coagulopathies, compromising the genetic revolution by unequal access to care. Other ethical issues include patient autonomy, since physicians may be bypassed by direct-to-consumer testing and use of master-degreed genetic counselors with minimal clinical experience. Survivor guilt is a concern for genetic tests predicting cancer or other severe outcomes since relatives with negative tests may watch their family members test positive and face dire consequences. Genetic testing must also balance confidentiality with needs of at-risk relatives, although employment or workplace discrimination has been addressed by the Genetic Information Nondiscrimination Act (GINA).
RR, Surgery: Ethical concerns that originally arose with genetic testing related to discrimination by insurance companies and employers have been resolved via legal action and pose no problems in current practice. Surgical management, however, poses a dilemma of timing of surgery. There is no data to suggest an appropriate age for prophylactic surgery. Of course, the goal is to achieve prophylaxis before cancer occurs. BRCA2 carriers tend to develop ovarian cancers at a later age than BRCA1 carriers,9 which we use as a guide when counseling on family completion and timing of surgery. Some work has been done on freezing ova for later fertilization, but this has not been very successful and has its own ethical issues.
LK, Primary Care Practice: With health care approaching 20% of the gross national product, all health care expenditures need to be scrutinized—although we never ration health care “at the bedside.” While the use of any diagnostic test or therapeutic option should be grounded in evidence,24 newer genetic modalities have not yet met cost-effectiveness standards.25 The final decision should be predicated on the question: Will the results of this test change my clinical management of this patient? Ultimately, care should be predicated on primum non nocere or “First, do no harm.” ■
References
1.Wilson GN, Tonk VS. Medicine Gone Array. A Clinician’s Guide to Genetic Testing for Neonatal and other Child Specialties. Workshop syllabus presented at the Pediatric Academic Societies meeting, May 2013. Available by request by emailing golder.wilson@ttuhsc.edu.
2.Hardy J, Singleton A. Genomewide association studies and human disease. N Engl J Med. 2009;360:1759-1768.
3.Kraft P, Hunter DJ. Genetic risk prediction—are we there yet? N Engl J Med. 2009;360:1701-1703.
4.Nakamura Y. Pharmacogenomics and drug toxicity. N Engl J Med. 2008;358:1-3.
5.OMIM—Online Mendelian Inheritance in Man. Available at www.ncbi.nlm.nih.gov/omim.
6.Personalized medicine. Mayo Clinic. Available at http://mayoresearch.mayo.edu/center-for-individualized-medicine/personalized-medicine.asp.
7.Gruppen LD, Palchik NS, Wulf FM, et al. The contribution of different components of the clinical encounter in generating and eliminating diagnostic hypothesis. Res Med Education. 1988;27;242-247.
8.National Comprehensive Cancer Network. Genetic/Familial High-Risk Assessment: Breast and Ovarian V. Fort Washington, PA; 2007.
9.Kobayashi H, Ohno S, Sasaki Y, Matsuura M. Hereditary breast and ovarian cancer susceptibility genes (Review). Oncol Rep. 2013; Jun 19. (Epub ahead of print)
10.Sparano JA, Fazzari MJ, Childs G. Clinical application of molecular profiling in breast cancer. Future Oncol. 2005;1:485-496.
11.Wilson BJ, Qureshi N, Santaguida P, et al. Systematic review: family history in risk assessment for common diseases. Ann Intern Med. 2009;151:878-885.
12.Feero WG. Personalized medicine with a genomic twist. ACP Internist. 2008 Jan.
13.Vig HS, Armstrong J, Egleston BL, et al. Cancer genetic risk assessment and referral patterns in primary care. Genet Test Mol Biomarkers. 2009;13:735-741.
14.GeneTests. Available at www.genetests.org.
15.Myriad genetics. Available at www.myriadtests.com.
16.Boughey JC, Hartmann LC, Anderson SS et al. Evaluation of the Tyrer-Cuzick (International Breast Cancer Intervention Study) model for breast cancer risk prediction in women with atypical hyperplasia. J Clin Oncol. 2010;28:3591-3596.
17.U.S. Preventive Services Task Force (USPSTF): An Introduction. Agency for Healthcare Research and Quality. 2012 Sep. Available at www.ahrq.gov/clinic/uspstfix.htm.
18.McCahon D, Holder R, Metcalfe A, et al. General practitioners’ attitudes to assessment of genetic risk of common disorders in routine primary care. Clin Genet. 2009:76:544-551.
19.Lieberman DA. Screening for colorectal cancer. N Engl J Med. 2009;361:1179-1187.
20.U.S. Preventive Services Task Force (USPSTF): Screening for Breast Cancer. Agency for Healthcare Research and Quality. 2008 Jan. Available at http://www.ahrq.gov/clinic/3rduspstf/Breastcancer/
21.Than MP. Communicating diagnostic uncertainties to patients: the problem of explaining unclear diagnosis and risk. Evid Based Med. 2009;14:66-67.
22.James PA, Harris M, Lindeman GJ, Mitchell G. Towards more effective and equitable genetic testing for BRCA1 and BRCA2 mutation carriers. J Med Genet. 2008;45:765-766.
23.Couzin J. Genetics. DNA test for breast cancer risk draws criticism. Science. 2008;322:357.
24.Ramsey SD, Veenstra DL, Garrison LP Jr, et al. Towards evidence-based assessment for coverage and reimbursement of laboratory-based diagnostic and genetic tests. Am J Manag Care. 2006;12:197-202.
25.Meckley LM, Neumann PJ. Personalized medicine: factors influencing reimbursement. Health Policy. 2010;94:91-100.