
A 2-year-old girl was seen by her pediatrician because of a 3-day history of runny nose, cough, congestion, and low-grade fevers. A viral upper respiratory tract infection was diagnosed and supportive care was recommended. The child returned 2 days later with persistent cough, mild tachypnea, and an episode of vomiting. The cough and tachypnea prompted the pediatrician to order a chest film, which revealed an enlarged cardiac silhouette.
The patient's medical history was unremarkable except for pneumonia, which had developed when she was 6 months old, and lack of any weight gain in the 6 months before the current illness. The family medical history was noncontributory, but all household members were experiencing a "flu-like" illness.
_________________________________________________________________________________________________________________________________________
Related Content
Aberrant Right Subclavian Artery
Pneumonia: Update on Causes--and Treatment Options
__________________________________________________________________________________________________________________________________________
The patient was referred to our tertiary care facility for further evaluation of the enlarged heart.
At presentation to our institution, the physical examination revealed an irritable, afebrile child weighing 11.1 kg (5th percentile) with obvious clear rhinorrhea. Her heart rate was 165 beats per minute, with good pulse volume; blood pressure, 103/60 mm Hg; respiratory rate, 28 breaths per minute; and oxygen saturation measured by pulse oximetry, 92% on room air. The patient had mild subcostal retractions and displayed jugular venous distention when propped at a 45-degree angle. The liver was palpable 5 cm below the right costal margin. Lungs were clear to auscultation.
A 3/6 systolic murmur was heard at the apex that radiated to the back. An S3 gallop was present. An ECG revealed sinus tachycardia, bilateral atrial enlargement, bilateral ventricular hypertrophy with strain, q wave in aVL, and a prolonged PR interval (0.16 to 0.22 second).

The chest film revealed severe cardiomegaly with clear lung fields (Figure 1). An echocardiogram showed severe mitral regurgitation, severe left atrial enlargement, and left ventricular enlargement with normal ventricular function. There was no tricuspid regurgitation and no aortic stenosis or coarctation. The right coronary artery was visualized, but not the left.
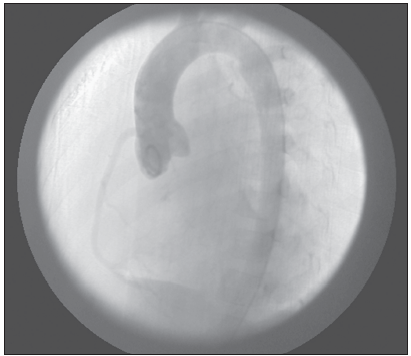
Cardiac catheterization revealed a single anterior coronary artery (the right coronary artery) arising from the aorta and an aberrant left coronary artery arising from the pulmonary artery (Figure 2).
The child underwent surgery. Intraoperatively, the papillary muscles were found to be infarcted and chordae foreshortened, which led to deformity of the edge of the mitral valve. The valve was replaced with a St Jude prosthetic mitral valve.
The child is currently being monitored by a cardiologist and a cardiovascular surgeon and is thriving.
ALCAPAAnomalous origin of the left coronary artery from the pulmonary artery (mostly the main pulmonary artery) (ALCAPA) occurs in roughly 1 of 300,000 births.1 Patients typically present in the first few months of life as pulmonary artery pressures fall, resulting in decreased blood flow and myocardial ischemia. The mitral papillary muscles are particularly sensitive to ischemia and damage.
 ALCAPA is diagnosed later in childhood in those who have better collateral circulation from the right coronary artery, which arises appropriately from the aorta. Those affected present with murmur and severe cardiomegaly. Findings of congestive heart failure are apparent. Patients without severely affected mitral valves present with dilated cardiomyopathy characterized by predominant left ventricular dysfunction and dilatation. ALCAPA can also present as sudden death.
ALCAPA is diagnosed later in childhood in those who have better collateral circulation from the right coronary artery, which arises appropriately from the aorta. Those affected present with murmur and severe cardiomegaly. Findings of congestive heart failure are apparent. Patients without severely affected mitral valves present with dilated cardiomyopathy characterized by predominant left ventricular dysfunction and dilatation. ALCAPA can also present as sudden death.
This entity should be first suspected with the abnormal physical examination findings of tachycardia, tachypnea, murmur, hepatomegaly, and an enlarged heart on chest radiographs. An ECG may show evidence of myocardial ischemia in the anterolateral leads with deep q waves in leads I and aVL. Echocardiographic features may include left ventricular dilatation and dysfunction. The aberrant coronary artery may be visualized arising from the pulmonary artery. In those patients with good collateral flow, the right coronary artery is dilated and may be tortuous. Retrograde flow in the left coronary artery can be demonstrated using color Doppler. Mitral insufficiency and valve abnormalities are also commonly found. Coronary angiography remains the gold standard for diagnosis when there is any doubt.
Acute treatment consists of cardiopulmonary stabilization. Among surgical interventions, re-implantation of the left coronary artery into the aorta and creation of an intrapulmonary tunnel that connects the anomalous artery to the aorta (the Takeuchi procedure) is most commonly employed.1 Improved blood flow to the myocardium often leads to dramatic improvement in left ventricular function. Valve replacement is necessary when mitral insufficiency is severe.