
A 17-year-old Asian male with no significant medical history presented to the emergency department (ED) with acute shortness of breath and associated left-sided chest pain. Symptoms began while the patient was at rest: the pain was sharp and worsened with inspiration. He denied a history of fever, trauma, cough, or any other constitutional complaints.
 In the ED, the patient's temperature was 37.8°C (100°F); heart rate was 100 beats per minute; respiratory rate, 28 breaths per minute; and blood pressure, 124/96 mm Hg. Oxygen saturation was 100% on room air. He had no nasal flaring but used accessory respiratory muscles. The trachea was in midline. Breath sounds were markedly diminished on the left side, with good air entry on the right. No crepitus, wheezing, stridor, or crackles were appreciated. Cardiac examination revealed a normal S1 and S2, without any murmurs, rubs, or gallops. Mediastinal shift could not be detected clinically. Chest films showed a left-sided tension pneumothorax (Figure 1).
In the ED, the patient's temperature was 37.8°C (100°F); heart rate was 100 beats per minute; respiratory rate, 28 breaths per minute; and blood pressure, 124/96 mm Hg. Oxygen saturation was 100% on room air. He had no nasal flaring but used accessory respiratory muscles. The trachea was in midline. Breath sounds were markedly diminished on the left side, with good air entry on the right. No crepitus, wheezing, stridor, or crackles were appreciated. Cardiac examination revealed a normal S1 and S2, without any murmurs, rubs, or gallops. Mediastinal shift could not be detected clinically. Chest films showed a left-sided tension pneumothorax (Figure 1).
A chest tube was placed, and symptoms resolved (Figure 2). The patient underwent surgery to resect an apical pleural bleb.
SPONTANEOUS PNEUMOTHORAX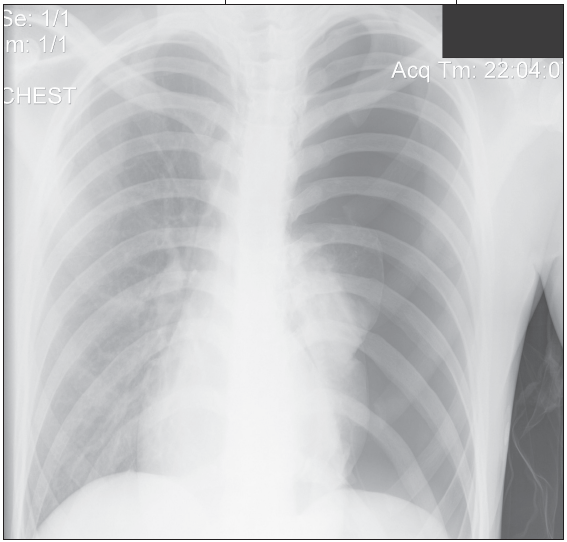 A spontaneous pneumothorax (SP) is a collection of air or gas between the visceral and parietal pleura that causes the lung to collapse in the absence of a traumatic injury to the chest or lung. Primary spontaneous pneumothorax (PSP) occurs in persons with no previously known lung disease. Typically, the cause of this type of pneumothorax is the rupture of a subpleural bleb or cyst in the lung.
A spontaneous pneumothorax (SP) is a collection of air or gas between the visceral and parietal pleura that causes the lung to collapse in the absence of a traumatic injury to the chest or lung. Primary spontaneous pneumothorax (PSP) occurs in persons with no previously known lung disease. Typically, the cause of this type of pneumothorax is the rupture of a subpleural bleb or cyst in the lung.
A secondary spontaneous pneumothorax (SSP) occurs in persons with known lung disease--most often chronic obstructive pulmonary disease in adults. In pediatric patients, cystic fibrosis, pneumonia, and asthma are the most common causes of SSP. Other conditions less commonly associated with SSP are tuberculosis, cystic adenomatoid malformation, Marfan syndrome, and certain types of interstitial lung disease.
SSP is generally more severe than PSP--and is often life threatening. Mortality associated with SSP is about 15%.1
Smoking greatly increases the risk of SP.2 Men who smoke a pack a day or less have a 20-fold increased risk of SP; in women, the risk rises by 10-fold. In men who smoke more than a pack per day, the risk of SP increases more than 80-fold; in women, the risk increases more than 40-fold.
SP also can be an inherited disorder, although this is not common. One literature review described 61 cases of familial SP in 22 families.3
SYMPTOMSThe major symptom is sudden-onset chest pain with breathlessness. This pain may be dull, sharp, or stabbing; it typically begins suddenly while the patient is at rest. Pain can be associated with dyspnea, tachypnea, and hypoxia; typically, it is exacerbated by breathing deeply or by coughing.
Patients with SSP may also experience dyspnea disproportional to the size of the pneumothorax as well as tachycardia, hypotension, and cyanosis.
DIAGNOSIS AND MANAGEMENTThe diagnosis usually can be made after a detailed history and physical examination. Chest radiographs can confirm the diagnosis and determine the size of the pneumothorax. A recent randomized controlled trial found no advantage for inspiratory/expiratory films.4
The objectives of management are to eliminate the intrapleural air collection, to facilitate pleural healing, and to prevent recurrence. The treatment of SP is multifactorial and depends on its size, course, and classification. A small pneumotho-rax may resolve spontaneously. Needle decompression or chest tube placement may be needed to facilitate reexpansion when air accumulation is relatively large. Strong- ly consider therapeutic interventions for patients with recurrent pneumo- thorax.
While the treatment options for PSP and SSP are the same, the conditions are managed differently. In asymptomatic patients with PSP who have less than 15% air accumulation, simple observation and administration of 100% oxygen have been successfully used as a treatment option.1 Oxygen increases the resorption rate of the pneumothorax 3-fold to 4-fold; the greatest increases occur in patients with larger pneumothoraces. The application of oxygen creates a gas pressure gradient between the pleural space and the tissue capillaries that surround the pleural space. This enhances the absorption of nitrogen and other gases within this space.5
If the pneumothorax is smaller than 15% and if the patient is symptomatic but hemodynamically stable, needle aspiration is considered the treatment of choice. Advantages include its relative simplicity and lack of invasiveness.6
SSP, on the other hand, can be life-threatening. Most patients are treated with a chest tube. Tube thoracostomy has been advocated for patients with PSP in whom simple aspiration fails--and for most patients with SSP.1,6 Other more invasive management options include pleural sclerosis (pleurodesis) and video-assisted thoracic surgery (VATS).
RECURRENCERecurrence rates can be high, espeically if SP is untreated. Recurrence rates as high as 30% at 6 months and 50% at 2 years have been reported.1 More specifically, recurrence rates have been reported at 28% for PSP and 53% for SSP.1 There is a 15% rate of recurrence on the contralateral side in patients with PSP. Recurrence is more likely in patients who are tall and thin and who smoke; however, there is no relationship with the number or size of apical blebs on CT. Once a recurrence has occurred, the risk for repeated pneumothoraces exceeds 50%.7
Chest tube insertion helps relieve the pneumothorax and improve symptoms. However, it does not reduce the risk of recurrence as significantly as VATS or pleurodesis. One randomized trial compared simple needle aspiration with tube thoracostomy in the management of first-time PSP.8 Recurrence rates were measured at 1 week (11% vs 12%), at 3 months (15% vs 8%), at 1 year (22% vs 42%), and at 2 years (31% vs 25%). There were no statistically significant differences between the 2 treatment modalities.
LONG-TERM CAREPatients who have had SP need to stop smoking and to avoid high altitudes, scuba diving, or flying in an unpressurized aircraft in attempt to limit the risk of a recurrent pneumothorax.
TAKE-HOME MESSAGECardiac causes of pediatric chest pain are uncommon. If the pain is associated with shortness of breath, especially in a thin adolescent who smokes, consider spontaneous pneumothorax (SP). When SP is diagnosed, it is important to differentiate between a primary and secondary cause because management differs.