
Cystic Hygroma in a Toddler

The parents of this 1-year-old girl brought her for evaluation of a neck mass of sudden onset (A). They had first noticed the mass on the morning of presentation. The child had cold symptoms and had been snoring, but she had no history of fever, shortness of breath, wheezing, or stridor. Her activity level and appetite had not changed.
The child was in no distress. Temperature was 38.1°C (100.5°F); heart rate, 156 beats per minute; respiration rate, 30 breaths per minute; oxygen saturation on room air, 99%; and weight, 8 kg. A cystic mass with a firm center was palpated on the right side of the neck. It was mobile and nontender; there was no erythema or warmth. Other physical findings were unremarkable.
The white blood cell count was 16,100/µL; hemoglobin level, 11.6 g/dL; hematocrit, 35.3%; and platelet count, 488,000/µL, with 56% segmented neutrophils, 0% bands, and 38% lymphocytes. The C-reactive protein level was 2.5 mg/L (normal, 0.0 to 0.9 mg/L); erythrocyte sedimentation rate was 24 mm/h (normal, 0 to 10 mm/h). Electrolyte levels were within normal limits.
The lesion's sudden onset--despite the lack of tenderness, warmth, or erythema--suggested an inflammatory or infectious cause and made cancer unlikely. The differential diagnosis of a neck mass also includes congenital malformations, such as a thyroglossal duct cysts, branchial apparatus cysts, dermoid cysts, and lymphatic malformations.1 The location of the swelling narrows the diagnostic possibilities (Table).2

This fetal malformation typically develops subcutaneously in the head and neck region and axilla. The lesion consists of massively dilated cystic lymphatic spaces that are lined by endothelial cells and separated by a small amount of intervening connective-tissue stroma, which often contains lymphoid aggregates. Histologically, these findings can be distinguished from capillary channels only by the absence of blood cells. Because the margins of the tumor are not discrete and the lesion is nonencapsulated, removal can be difficult.1
Surgical excision has been the most accepted therapy. Complete excision without sacrificing healthy structures is the goal. For lesions that infiltrate the facial nerve or other vital structures, watchful waiting may be appropriate. Definitive therapy can be delayed until the child is several years old. However, prompt removal of lymphangiomas is necessary when there is potential for airway obstruction--which is highest in tumors of the sublingual, submandibular, or minor salivary glands. Tracheotomy may be required if the lymphangioma cannot be removed completely. Lymphagiomas rarely recur when all of the gross tumor is removed; however, recurrence has been reported in about 15% of patients with residual disease.3
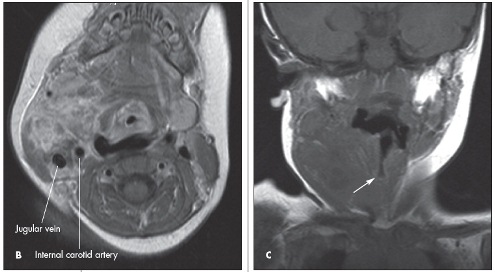
Ultrasonography is a reasonable first step in the evaluation of a neck mass. In this case, the child was referred to us after she was seen at another hospital where CT was performed. The CT scans revealed a cystic-density lesion that occupied multiple spaces in the right side of the neck with effacement of the vasculature and tracheal air column. These findings were limited, however, because the child was unable to remain immobile during the imaging. She subsequently underwent MRI under sedation. Scans showed a 3.3 × 2.9-cm, multiloculated cystic mass that extended the entire length of the neck above the supraclavicular region (B). The mass displaced the vascular structures posteriorly. The airway was displaced slightly to the left because of mass effect (C, arrow). These findings indicated a cystic hygroma.
A nonsurgical treatment option, OK-432 (Picibanil) sclerotherapy, has been shown to reduce the size of the mass or obliterate it completely.4
The cystic hygroma in this child, although it seemed acute, was probably always present and had become larger as a result of an upper respiratory tract infection--the suspected cause of her cold symptoms. She was given antibiotic therapy for the infection. The mass was not excised because of possible complications with the surrounding structures. Removal may be necessary if the mass does not regress after the current infection resolves, if the mass grows larger, or if it causes a respiratory problem.