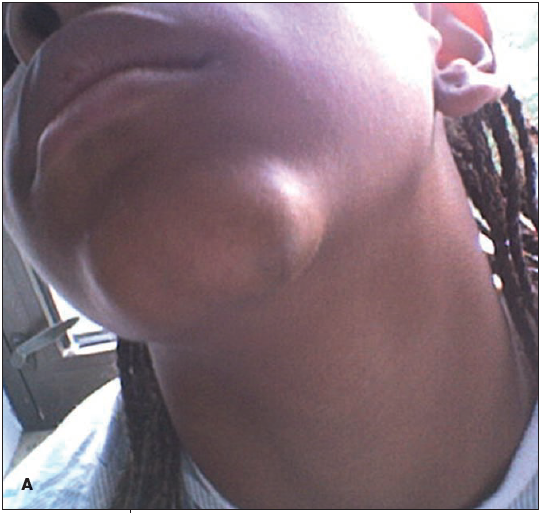
An 11-year-old girl presented with a swelling on the left side of the chin of 1 month's duration; in the past 24 hours, following a bite by an unidentified insect, the swelling had rapidly enlarged and become painful (A). She was otherwise healthy and had no significant medical or family history.
The mass was soft, fluctuant, tender to palpation, and nonerythematous; there was no discharge. Needle aspiration revealed no fluid, and the patient was scheduled for incision and drainage the next day. However, an ultrasonogram revealed a heterogeneous complex mass, suggestive of an abscess or tumor. Further evaluation with an MRI scan showed an anterior subcutaneous mass abutting the left mandible, suggestive of a vascular lesion. The patient was given oral cephalexin and scheduled for excision biopsy.
A soft, nonvascular, 2.1× 1.4-cm mass with about 1 cm of surrounding tissue was excised (B); there was no bony involvement. On gross examination, the contents of the mass were whitish tan and watery, resembling dishwater. Pathological findings were diagnostic of cystic hygroma. Microscopically, the lesion had large, irregular- shaped spaces lined by bland, flattened endothelial cells in a fibrous stroma with flocculent, eosinophilic proteinaceous material (C).


Cystic hygroma, also known as lymphangioma, may develop in the mediastinum, axilla, or-as in this case-in the soft tissue of the neck.Its onset is most common in utero and in early infancy. The incidence of cystic hygroma is between 1 in 6000 and 1 in 16,000 (although some suggest that these low numbers do not account for intrauterine cases, which are often undiagnosed).1,2 About 50% to 65% of all cystic hygromas are present at birth, 80% to 90% are diagnosed by the end of the second year of life,1,3,4 and only 6% to 10% are found in children older than 10 years.5 The origin of cystic hygromas is somewhat unclear; they may be associated with a genetic disorder, such as Turner syndrome, trisomy (13, 18, or 21), or Noonan syndrome,2 or they may develop secondary to an environmental factor (such as viral infection or maternal substance abuse or ethanol abuse) or for unknown reasons.6
The differential diagnosis of this patient's chin mass included, in addition to cystic hygroma, chin abscess, brachial cleft cystic lesion, lymphadenitis, and teratoma. Because the classic manifestation of cystic hygroma-a soft, compressible, transilluminating, loculated, illdefined mass that is not attached to the skin but movable across deeper tissues-is not always present, diagnosis based on clinical findings alone is unreliable.7 Results of CT, MRI, or ultrasonography can help define the relationship between the lesion and neighboring structures. However, only pathological examination of the excised mass can definitively confirm the diagnosis.
Although some studies advocate conservative treatment of cystic hygroma (via aspiration or sclero-therapy with streptococcal extract OK-432 or other agents),1,8 surgical excision is considered the standard of care. Statistics show recurrence of complex masses in 10% to 27% of cases2,9 after complete excision and in 30% to 100% of cases after sclerotherapy8 or partial excision.9 Because of the high risk of injury associated with surgical excision of cystic hygromas that are attached to underlying anatomy, complete excision need not be pursued when there is risk of damage to surrounding structures.
The cystic hygroma in this patient was unusual in that it became symptomatic at an older age, seemingly after an insect bite. The bite may have resulted in mild infection that caused the mass to enlarge. Because the mass was not attached to any underlying structures, complete removal was possible. Five months after surgery, the patient was asymptomatic, the incision sites had healed well, and there were no signs of recurrence.