
Delirium in Hospitalized Older Patients
Introduction
Delirium, defined as an acute confusional state with change in attention and cognition, is a common condition that results in significant morbidity and mortality among elderly persons. It is characterized by disturbances of consciousness, reduced environmental awareness, and a waxing and waning course. Ten percent to 31% of geriatric patients presenting to an emergency department have delirium and 6% to 56% of older patients develop this complication during hospitalization.1 Delirium results in many adverse outcomes, including increased length of hospitalization, impaired physical and cognitive recovery at 6 and 12 months, and mortality rates that are twice as high as that of age-matched control patients.2 Despite the common nature and significant consequences of delirium, up to 70% of delirium cases in hospitalized elderly persons are unrecognized.3
Risk Factors
 Delirium is almost always multifactorial in origin, resulting from baseline vulnerability and precipitating factors. Predisposing factors that increase baseline vulnerability include advanced age, impaired cognitive status, impaired functional status, sensory impairment, medical illnesses such as central nervous system disease, and exposure to certain medications.4 Precipitating factors for delirium include neurologic/central nervous system disease, metabolic derangements, trauma, cancer, surgery, illness, environmental insults, pain, and medication issues, including polypharmacy and the use of certain precipitating medications. (See Table I for a list of medications that are associated with the development of delirium.) Alcohol and substance withdrawal are common contributors to delirium and should be considered in all patients. In older persons, minimal insults may result in delirium, as many patients have multiple predisposing baseline factors.
Delirium is almost always multifactorial in origin, resulting from baseline vulnerability and precipitating factors. Predisposing factors that increase baseline vulnerability include advanced age, impaired cognitive status, impaired functional status, sensory impairment, medical illnesses such as central nervous system disease, and exposure to certain medications.4 Precipitating factors for delirium include neurologic/central nervous system disease, metabolic derangements, trauma, cancer, surgery, illness, environmental insults, pain, and medication issues, including polypharmacy and the use of certain precipitating medications. (See Table I for a list of medications that are associated with the development of delirium.) Alcohol and substance withdrawal are common contributors to delirium and should be considered in all patients. In older persons, minimal insults may result in delirium, as many patients have multiple predisposing baseline factors.
Pathogenesis
Although the risk factors for delirium are well defined, the pathogenesis is less clearly understood. Multiple pathogenic mechanisms are most likely involved in delirium development, with neurotransmitters and inflammation playing an important role. Cholinergic deficiency and dopaminergic excess have been strongly correlated with delirium development, but norepinephrine, serotonin, gamma-aminobutyric acid, glutamate, and melatonin imbalances may also contribute.4 Cytokines also appear to be involved in the pathogenesis of delirium by increasing the permeability of the blood-brain barrier and altering neurotransmission.4,5 In particular, decreased levels of somatostatin have been documented in patients with delirium who had no overt central nervous system disease.6,7 The activation of the sympathetic nervous system and hypothalamic-pituitary-adrenocortical axis caused by the stress of illness or trauma may also contribute to the development of delirium by adverse effects on hippocampal serotonin receptors.4
Diagnosis
Delirium is a clinical diagnosis, and the healthcare provider must be familiar with the typical features of delirium to make an accurate diagnosis. In the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), the diagnostic criteria for delirium due to multiple etiologies are defined as follows8:
(1) Disturbance of consciousness with reduced ability to focus, sustain, or shift attention;
(2) Change in cognition or the development of a perceptual disturbance that is not better accounted for by a preexisting, established, or evolving dementia;
(3) The disturbance develops over a short period of time and tends to fluctuate during the course of the day;
(4) There is evidence from the history, physical examination, or laboratory findings that the delirium has more than one etiology.8
As noted previously, the development of delirium in elderly patients is almost always secondary to multiple etiologies.
 The Confusion Assessment Method (CAM) is the most widely used and validated assessment tool for the bedside diagnosis of delirium (Table II).9 It evaluates for the core components of delirium, including acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness. The CAM has a sensitivity of 94% to 100% and a specificity of 90% to 95%.9 Practical questions that can be used at the bedside to evaluate for attention include asking patients to recite the months of the year or days of the week backwards.
The Confusion Assessment Method (CAM) is the most widely used and validated assessment tool for the bedside diagnosis of delirium (Table II).9 It evaluates for the core components of delirium, including acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness. The CAM has a sensitivity of 94% to 100% and a specificity of 90% to 95%.9 Practical questions that can be used at the bedside to evaluate for attention include asking patients to recite the months of the year or days of the week backwards.
Other common clinical features of delirium include cognitive deficits, perceptual disturbances including hallucinations, emotional disturbances, and alteration of the sleep-wake cycle. Psychomotor disturbances are also common in delirium, and patients may manifest a hyperactive, hypoactive, or mixed presentation. The presentation of hyperactive delirium ranges from restlessness to constant movement and agitation. Hypoactive delirium may present as slowed movement, paucity of speech, or even unresponsiveness. Hypoactive delirium is less likely than hyperactive delirium to be recognized by healthcare providers and is associated with higher mortality at 6 months and 1 year.10,11 Patients with mixed delirium manifest characteristics of both hyperactive and hypoactive delirium.
All hospitalized elderly patients should be assessed for delirium on a daily basis. It is optimal if this assessment is done two or three times throughout the day to monitor for developing changes in mental status. If delirium is diagnosed, it is important to identify and address causative factors. Initial evaluation should include a thorough physical examination that includes a review of the patient’s vital signs. Basic workup includes a complete blood count, serum chemistries, thyroid function studies, urinalysis and urine culture, and chest radiography. Depending on the individual patient, electrocardiography, lumbar puncture, blood cultures, urine toxicology, cardiac enzymes, arterial blood gas, and a blood alcohol level may be warranted. Neuroimaging with computed tomography is generally not indicated unless the patient has focal neurologic findings on examination, a history of head trauma, or fever associated with encephalopathy, or unless no other cause of the delirium can be determined.12 All medications should be carefully reviewed with the understanding that even long-standing, previously well-tolerated medications can contribute to delirium in the setting of precipitating factors during hospitalization. It is also important to assess for illicit drug and alcohol use, as withdrawal can contribute to delirium.
Prevention
Predictive Models
Primary prevention measures should be employed in hospitalized elderly patients to reduce the frequency and subsequent complications of delirium. Although all hospitalized older persons should be screened for delirium, predictive models are useful for identifying those patients who are at particularly high risk. Four independent baseline risk factors have been identified as predictors for delirium among elderly hospitalized patients on a medical service: vision impairment; severe illness (a composite of nurse rating and an Acute Physiology and Chronic Health Evaluation II [APACHE II] score of more than 16); cognitive impairment, defined as a Mini-Mental State Examination (MMSE) score of less than 24; and an elevated blood urea nitrogen (BUN) to creatinine ratio of 18 or higher.13 A risk stratification system was developed by Inouye et al13 that assigned 1 point for each risk factor. Subjects with no points had a low risk (3%-9%) of delirium, while those with 3 to 4 points had the highest risk of delirium (32%-83%).13
Predictive models have also been developed for elderly surgical patients. In a study by Marcantonio et al,14 postoperative delirium was associated with the following independent correlates among older persons who underwent noncardiac surgery: age 70 years or older; alcohol abuse; cognitive impairment as determined by the Telephone Interview for Cognitive Status; severe physical functional impairment as determined by the American Society of Anesthesiologists physical status classification system; markedly abnormal serum sodium, potassium, or glucose level; noncardiac thoracic surgery; and aortic aneurysm surgery. Subjects with no risk factors had a 2% rate of postoperative delirium, and this increased to 50% in subjects with three or more risk factors. In a more recent study by Rudolph et al,15 four variables were associated with postoperative delirium among patients age 60 years or older who were undergoing cardiac surgery: low MMSE score (≤ 23 = 2 points, 24-27 = 1 point); history of cerebrovascular accident/transient ischemic attack (1 point); high Geriatric Depression Scale score (> 4 = 1 point); and abnormal albumin level (1 point).15 As compared with subjects with no points, having 1 point more than doubled the risk of postoperative delirium and having 3 or more points more than quadrupled this risk. In yet another study, patients age 70 years and older who were undergoing hip surgery were assigned 1 point for each of the following delirium risk factors: binocular near vision worse than 20/70 following correction; severe illness, defined as an APACHE II score of higher than 16; MMSE score below 24; or dehydration, as indicated by a BUN to creatinine ratio of 18 or higher.16 Subjects with none of these risk factors were classified as low risk, those with one or two risk factors were classified as intermediate risk, and those with three or four risk factors were classified as high risk. Incidence of postoperative delirium was 3.8% in the low-risk group, 11.1% in the intermediate-risk group, and 37.1% in the high-risk group (P < 0.001; relative risk, 98). Researchers reported that cognitive impairment at admission had the highest predictive value for the development of delirium.16
Nonpharmacologic Prevention
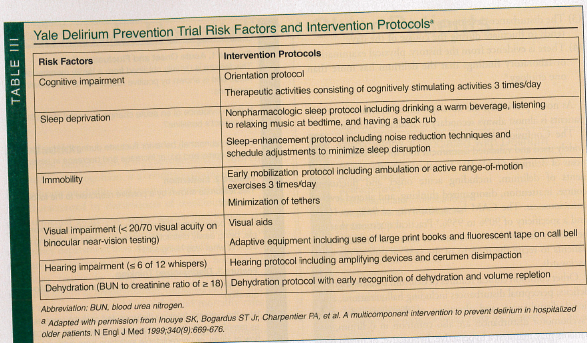
Since most cases of delirium are multifactorial, multicomponent prevention strategies are most effective in preventing this condition. The Yale Delirium Prevention Trial implemented standard protocols directed at addressing six risk factors for delirium: cognitive impairment; sleep deprivation; immobility; visual impairment; hearing impairment; and dehydration (Table III).17 Standardized intervention protocols for the management of these risk factors resulted in a significant reduction in the development of delirium, from 15% in the usual-care group to 9.9% in the intervention group. In addition, the number and duration of delirium episodes among older persons in the intervention group were significantly reduced; however, the interventions had no significant effect on the severity or the recurrence of delirium.17 The interventions employed in the Yale Delirium Prevention Trial were adapted as the Hospital Elder Life Program (HELP), which has been implemented in hospitals throughout the United States, Canada, and Australia. Often implemented mainly by volunteers to minimize financial investment, this program is cost-effective when used in patients who are at intermediate risk for developing delirium. 18 Cost savings among intermediate-risk subjects were primarily due to savings on nursing costs, diagnostic procedures, and other cost components, including coronary and intensive care units, hospital supplies, surgical and postsurgical costs, rehabilitation services, and physical therapy. Cost-effectiveness was not demonstrated among high-risk subjects.18
In a prospective, randomized trial of patients age 65 years and older, proactive geriatric consultation was found to be successful in preventing postoperative delirium in patients with hip fractures.19 Geriatricians evaluated patients daily during their hospitalization and made targeted, protocol-based recommendations, including the treatment of pain, elimination of unnecessary medications, regulation of bowel and bladder function, and early mobilization. Delirium occurred in 32% of subjects in the intervention group as compared with 50% of subjects in the usual-care group. Overall, geriatric consultation reduced the incidence of delirium cases by one-third and severe delirium cases by one-half.19
Pharmacologic Prevention
Several studies have focused on the pharmacologic prevention of delirium in postoperative patients. The effect of donepezil in reducing postoperative delirium after elective total hip replacement was evaluated in a randomized, double-blind, placebo-controlled trial of 33 elderly persons.20 Subjects in the intervention group received donepezil 5 mg daily for 4 days postoperatively. Donepezil did not significantly reduce the incidence of delirium or the length of hospitalization in these patients. Another study evaluated the impact of donepezil on delirium prevention in patients age 50 years or older who were undergoing elective knee or hip arthroplasty.21 Subjects in the intervention group took donepezil 5 mg daily for 14 days prior to surgery to obtain a steady state, and continued on the medication for 14 days postoperatively. The investigators found no difference in the incidence or the duration of delirium among the intervention and control groups.21
In a recent study, Gamberini et al22 evaluated the use of rivastigmine for the prevention of postoperative delirium in 120 patients, age 65 years or older, following elective cardiac surgery. Subjects in the intervention group received rivastigmine 1.5 mg 3 times daily from the evening before surgery until the evening of postoperative day 6. No significant difference in incidence, duration, or severity of delirium was found between the intervention and control groups.22 The effect of haloperidol prophylaxis has been evaluated in patients, age 70 years and older, undergoing hip surgery.23 Subjects in the intervention group received haloperidol 0.5 mg 3 times daily from hospital admission until postoperative day 3. Proactive geriatric consultation was also provided to all patients. Haloperidol was not effective in reducing the incidence of postoperative delirium; however, it is important to note that the duration and severity of delirium and the length of hospitalization was significantly reduced in the intervention group.23
Management
Successful delirium management includes addressing the underlying causes, providing supportive care, and treating behavioral symptoms. Delirium should be considered a medical emergency because of the associated morbidity and mortality, and it often occurs in the setting of significant medical illness. Initial management should focus on ensuring stability of the patient by assessing respiratory and circulatory stability and evaluating for possible life-threatening causes, including myocardial infarction, cerebrovascular accident, or infection. Subsequent supportive care should include maintaining adequate nutrition and hydration; frequent repositioning and early mobilization to prevent pressure ulcers; deep vein thrombosis prophylaxis; minimizing the use of tethers, including Foley catheters; and avoiding the use of physical restraints. Nonpharmacologic measures are first line in the symptomatic treatment of delirium, and include reorienting the patient frequently, presence of the family at the bedside whenever possible, limiting staffing and room changes, and maintaining the sleep-wake cycle by minimizing nighttime interruptions and ensuring that the patient is awake and situated in a bright room during the daytime.
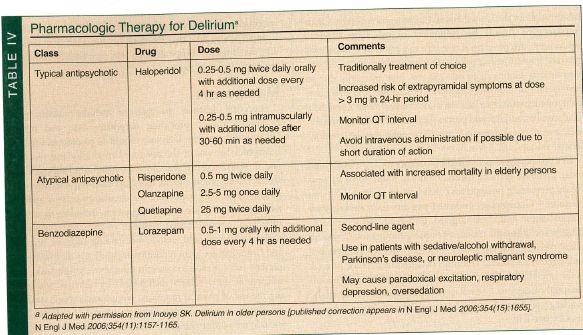
Pharmacologic treatment of delirium should only be used in patients whose symptoms place themselves or others at risk for harm. Haloperidol, a typical antipsychotic agent, has traditionally been the agent of choice for treating delirium. A randomized, double-blind trial comparing haloperidol, chlorpromazine, and lorazepam for the treatment of delirium in hospitalized patients with HIV infection found haloperidol to be superior to the other two medications in these patients.24 Specifically, haloperidol was effective in improving symptoms of delirium and was found to have a very low rate of extrapyramidal side effects. Chlorpromazine was also determined to be efficacious in reducing symptoms, while lorazepam was found to be ineffective and was associated with adverse effects.24 The efficacy rate of haloperidol is similar to that of atypical antipsychotic agents.25,26 Atypical antipsychotics are quite efficacious in treating the behavioral symptoms of delirium, with risperidone and olanzapine having an efficacy of 80% to 85% and 70% to 76%, respectively.25 Quetiapine has been less frequently studied, but also appears to be a reasonable treatment option. As compared with haloperidol, the atypical antipsychotics produced fewer adverse effects, including extrapyramidal symptoms.25
Typical and atypical antipsychotic medications carry black-box warnings from the Food and Drug Administration (FDA) regarding an increased risk of death when used in elderly patients treated for dementia-related psychosis.27 These warnings, issued for atypical antipsychotics in 2005 and typical antipsychotics in 2008, are supported by numerous studies. In a retrospective cohort study of 22,890 patients age 65 years or older, typical antipsychotics were associated with a significantly greater adjusted risk of death than atypical antipsychotics throughout the 180-day study period.28 The greatest increase in the adjusted risk of death for typical antipsychotics occurred within the first 40 days of therapy and when administered at higher doses. A population-based, retrospective cohort study that evaluated the use of antipsychotic agents and mortality among 27,259 community-dwelling adults and nursing home residents, age 66 years or older, with dementia found a statistically significant increased risk of death at 30 days among both community-dwelling participants and nursing home residents with new use of atypical antipsychotics. Typical antipsychotic use was associated with a higher risk of death throughout the 180-day study period.29 A recent study evaluating the impact of the FDA black-box warning for typical and atypical antipsychotic medication use found an overall decrease in usage; decreased usage was most significant for atypical antipsychotics in elderly patients with dementia.30
Despite the FDA warnings and study findings, antipsychotic medications are often used in elderly persons with delirium who present a risk to themselves or others. In these cases, healthcare providers should have a thorough discussion of the possible benefits and risks of antipsychotic therapy with the patient’s designated decision maker. Antipsychotics should be used in the lowest effective dose for the shortest duration possible.
Lorazepam is a second-line therapy for delirium and should be used only in patients with sedative/alcohol withdrawal, Parkinson’s disease, or neuroleptic malignant syndrome.4 Even among these select patients, however, lorazepam should be used with significant caution, as there is a risk of increased confusion and paradoxical excitement.
See Table IV for detailed information on pharmacologic therapy for the management of delirium.
Prognosis
Despite the use of appropriate management options, delirium continues to result in increased morbidity and mortality among a significant number of patients. Persistent delirium, defined as continued evidence of delirium at the time of hospital discharge, is more common among elderly persons, affecting approximately 39% of older patients.31 Following hospital discharge, 44.7% still had delirium at 1 month and 32.8% at 3 months. Independent risk factors for persistent delirium include baseline dementia, visual impairment, functional impairment, high comorbidity, and the use of physical restraints.32 Persistent delirium is associated with adverse outcomes. In a study of patients over age 65 years with hip fractures, delirium persisting 1 month after hospital discharge was associated with an increased decline in activities of daily living and ambulation, and an increased incidence of new nursing home placement or death as compared with similar subjects who did not have delirium.33 In a study of 433 participants age 70 years and older, 83.3% of patients with persistent delirium died or were admitted to a nursing home 1 year following hospitalization.34 Although these findings did not meet the criteria for statistical significance, they were clinically significant, as only 67.7% of subjects in whom delirium had resolved by discharge and 41.5% of subjects who never had delirium died or were admitted to a nursing home after 1 year of follow-up.34
While dementia has long been a well-recognized risk factor for delirium, it now appears that delirium may increase the risk for the development of cognitive dysfunction. In a study published in 2008 of subjects age 60 years or older who underwent elective, noncardiac surgery, delirium was associated with an increased incidence of early postoperative cognitive dysfunction 7 days postoperatively; however, there was no relationship found between postoperative delirium and long-term postoperative cognitive dysfunction at 3 months.35 In another study, an evaluation of patients who underwent cardiac surgery conducted 1 to 1.5 years after surgery did find a clinically—but not statistically—significant increase in the incidence of memory and concentration problems among subjects who developed postoperative delirium.36 A prospective study showed delirium to be associated with decreased MMSE scores 1 year after hospitalization, following adjustment for comorbidity, severity of illness, and other covariates, in patients age 65 years and older who were admitted to a medical service.37
Conclusion
Delirium affects up to 56% of hospitalized elderly patients,1 and often results in significant adverse outcomes, including increased length of hospitalization, decreased activities of daily living, increased incidence of institutionalization following hospitalization, and death. All geriatric patients should be evaluated for delirium at the time of hospital admission, and a delirium prevention program should be initiated for all patients. If delirium does develop, evaluation and treatment of causative factors should be implemented. Nonpharmacologic interventions, including frequent reorientation, family presence, and minimization of sleep-wake disturbances, are the basis of symptom management. Pharmacologic therapy is appropriate when symptoms of delirium place the patient or others at risk of harm. Haloperidol is the traditional first-line agent, but atypical antipsychotics have been determined to have similar efficacy.
The author reports no relevant financial relationships.
Dr. Botts is Director of Inpatient Services and Geriatric Education, Division of Gerontology, Beth Israel Deaconess Medical Center, and is Instructor of Medicine, Harvard Medical School, Boston, MA.
References
1. Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium in medical in-patients: A systematic literature review. Age Ageing 2006;35(4):350-364.
2. McCusker J, Cole M, Abrahamowicz M, Primeau F, Belzile E. Delirium predicts 12-month mortality. Arch Intern Med 2002;162(4):457-463.
3. Miller MO. Evaluation and management of delirium in hospitalized older patients. Am Fam Physician 2008;78(11):1265-1270.
4. Inouye SK. Delirium in older persons [published correction appears in N Engl J Med 2006;354(15):1655]. N Engl J Med 2006;354(11):1157-1165.
5. Cole MG. Delirium in elderly patients. Am J Geriatr Psychiatry 2004;12(1):7-21.
6. Broadhurst C, Wilson K. Immunology of delirium: New opportunities for treatment and research. Br J Psychiatry 2001;179:288-289.
7. Koponen HJ, Leinonen E, Lepola U, Riekkinen PJ. A long-term follow-up study of cerebrospinal fluid somatostatin in delirium. Acta Psychiatr Scand 1994;89(5):329-334.
8. Delirium, dementia, and amnestic, and other cognitive disorders. In: Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Text Revision. Washington, DC: American Psychiatric Association; 2000:135-147.
9. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990;113(12):941-948.
10. Kiely DK, Jones RN, Bergmann MA, Marcantonio ER. Association between psychomotor activity delirium subtypes and mortality among newly admitted post-acute facility patients. J Gerontol A Biol Sci Med Sci 2007;62(2):174-179.
11. Yang FM, Marcantonio ER, Inouye SK, et al. Phenomenological subtypes of delirium in older persons: Patterns, prevalence, and prognosis. Psychosomatics 2009;50(3):248-254.
12. Inouye SK. Delirium in hospitalized older patients. Clin Geriatr Med 1998;14(4):745-764.
13. Inouye SK, Viscoli CM, Horwitz RI, Hurst LD, Tinetti ME. A predictive model for delirium in hospitalized elderly medical patients based on admission characteristics. Ann Intern Med 1993;119(6):474-481.
14. Marcantonio ER, Goldman L, Mangione CM, et al. A clinical prediction rule for delirium after elective noncardiac surgery. JAMA 1994;271(2):134-139.
15. Rudolph JL, Jones RN, Levkoff SE, et al. Derivation and validation of a preoperative prediction rule for delirium after cardiac surgery. Circulation 2009;119(2):229-236.
16. Kalisvaart KJ, Vreeswijk R, de Jonghe JF, van der Ploeg T, van Gool WA, Eikelenboom P. Risk factors and prediction of postoperative delirium in elderly hip-surgery patients: Implementation and validation of a medical risk factor model. J Am Geriatr Soc 2006;54(5):817-822.
17. Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 1999;340(9):669-676.
18. Rizzo JA, Bogardus ST Jr, Leo-Summers L, Williams CS, Acampora D, Inouye SK. Multicomponent targeted intervention to prevent delirium in hospitalized older patients: What is the economic value? Med Care 2001;39(7):740-752.
19. Marcantonio ER, Flacker JM, Wright RJ, Resnick NM. Reducing delirium after hip fracture: A randomized trial. J Am Geriatr Soc 2001;49(5):516-522.
20. Sampson EL, Raven PR, Ndhlovu PN, et al. A randomized, double-blind, placebo-controlled trial of donepezil hydrochloride (Aricept) for reducing the incidence of postoperative delirium after elective total hip replacement. Int J Geriatr Psychiatry 2007;22(4):343-349.
21. Liptzin B, Laki A, Garb JL, Fingeroth R, Krushell R. Donepezil in the prevention and treatment of post-surgical delirium. Am J Geriatr Psychiatry 2005;13(12):1100-1106.
22. Gamberini M, Bolliger D, Lurati Buse GA, et al. Rivastigmine for the prevention of postoperative delirium in elderly patients undergoing elective cardiac surgery—A randomized controlled trial. Crit Care Med 2009;37(5):1762-1768.
23. Kalisvaart KJ, de Jonghe JF, Bogaards MJ, et al. Haloperidol prophylaxis for elderly hip-surgery patients at risk for delirium: A randomized placebo-controlled study.J Am Geriatr Soc 2005;53(10):1658-1666.
24. Breitbart W, Marotta R, Platt MM, et al. A double-blind trial of haloperidol, chlorpromazine, and lorazepam in the treatment of delirium in hospitalized AIDS patients. Am J Psychiatry 1996;153(2):231-237.
25. Ozbolt LB, Paniagua MA, Kaiser RM. Atypical antipsychotics for the treatment of delirious elders. J Am Med Dir Assoc 2008;9(1):18-28.
26. Han CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004;45(4):297-301.
27. U.S. Food and Drug Administration. Antipsychotics, conventional and atypical. http://www.fda.gov. Accessed November 15, 2010.
28. Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 2005;353(22):2335-2341.
29. Gill SS, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med 2007;146(11):775-786.
30. Dorsey ER, Rabbani A, Gallagher SA, Conti RM, Alexander GC. Impact of FDA black box advisory on antipsychotic medication use. Arch Intern Med 2010;170(1):96-103.
31. Cole MG, Ciampi A, Belzile E, Zhong L. Persistent delirium in older hospital patients: A systematic review of frequency and prognosis. Age Ageing 2009;38(1):19-26.
32. Siddiqi N, Stockdale R, Britton AM, Holmes J. Interventions for preventing delirium in hospitalised patients. Cochrane Database Syst Rev 2007;(2):CD005563.
33. Marcantonio ER, Flacker JM, Michaels M, Resnick NM. Delirium is independently associated with poor functional recovery after hip fracture. J Am Geriatr Soc 2000;48(6):618-624.
34. McAvay GJ, Van Ness PH, Bogardus ST Jr, et al. Older adults discharged from the hospital with delirium: 1-year outcomes. J Am Geriatr Soc 2006;54(8):1245-1250.
35. Rudolph JL, Marcantonio ER, Culley DJ, et al. Delirium is associated with early postoperative cognitive dysfunction. Anaesthesia 2008;63(9):941-947.
36. Koster S, Hensens AG, van der Palen J. The long-term cognitive and functional outcomes of postoperative delirium after cardiac surgery. Ann Thorac Surg 2009;87(5):1469-1474.
37. McCusker J, Cole M, Dendukuri N, Belzile E, Primeau F. Delirium in older medical inpatients and subsequent cognitive and functional status: A prospective study. CMAJ 2001;165(5):575-583.