
Eosinophilic Granuloma of Bone
 For 2 to 3 weeks, a 10-year-old boy had pain and swelling of the left ankle. He had no history of trauma, pain in other joints, fever, fatigue, or decreased appetite. The pain had gradually increased and limited his participation in recreational activities, such as soccer. Review of systems was otherwise unremarkable. Medical or surgical history was noncontributory.
For 2 to 3 weeks, a 10-year-old boy had pain and swelling of the left ankle. He had no history of trauma, pain in other joints, fever, fatigue, or decreased appetite. The pain had gradually increased and limited his participation in recreational activities, such as soccer. Review of systems was otherwise unremarkable. Medical or surgical history was noncontributory.
Vital signs were normal. Soft tissue swelling of the left foot and ankle was nonsignificant; there was no obvious deformity. Point tenderness was marked over the medial malleolus and over the shaft of the fifth metatarsal distally. The remaining physical findings were normal.
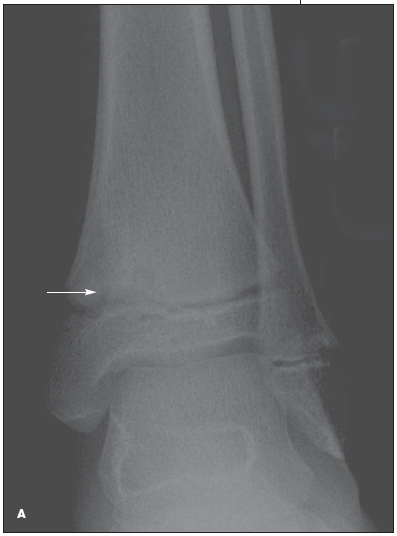
Radiographs revealed a 13-mm lytic lesion in the left distal tibia (A) and an 8-mm lytic lesion in the left fifth metatarsal (B). At this point, the differential diagnosis included tuberculosis, fungal infection (especially blastomycosis or coccidioidomycosis), primary bone tumor, and metastatic disease (rhabdomyosarcoma, neuroblastoma). Bone lesions in children should raise suspicion for a metastatic process. The lack of pulmonary findings made an infection, such as tuberculosis or blastomycosis, unlikely.

Further evaluation revealed a white blood cell count of 8600/μL; hemoglobin level, 13.7 g/dL; hematocrit, 39.2%; and platelet count, 399,000/μL. Electrolyte concentrations were within normal limits. Erythrocyte sedimentation rate was 23 mm/h; lactate dehydrogenase level, 226 U/L (normal, 90 to 250 U/L); and uric acid level, 4.3 mg/dL (normal, 2.5 to 8.0 mg/dL). A skeletal survey showed no other bone lesions. Findings on a CT scan of the chest, abdomen, and pelvis were normal. The patient underwent bone biopsy with aspiration of both lesions. Histological examination of the aspirate revealed eosinophilic granuloma. Results of staining for acid-fast bacilli and fungi and of bacterial culture of the aspirate were negative.
Eosinophilic granuloma of bone is relatively rare, with an incidence of 1 case per 2 million persons per year.1 The usual age at presentation is 5 to 10 years.2 Lesions can be monostotic (solitary) or polyostotic (multiple). The absence of extraskeletal involvement distinguishes this condition from Langerhans cell histiocytosis, which should be excluded because of the difference in treatment and less favorable prognosis.
Symptoms vary depending on the area of bone involved. They may include pain, swelling, or even pathological fractures. Occasionally, patients present with refractory otitis media (when the temporal bone is involved), proptosis (when the orbital bone is involved), or loose teeth (when the jaw is involved). Diagnosis requires bone biopsy with histological confirmation because the radiographic finding of a lytic lesion is associated with many other benign and malignant primary bone tumors. In fact, all primary bone tumors require bone biopsy for diagnosis.
Treatment options include observation of the lesions, bone graft and curettage, corticosteroid injection, and radiation therapy.3 The type of therapy depends on the location, size, and number of lesions. Spontaneous remission of solitary lesions is common. This patient underwent curettage of the larger tibial lesion and observation of the smaller lesion.