
HISTORY
 Ten-year-old girl assessed because of limitation of neck motion. Born at term to non-consanguineous parents. No history of necktrauma. Family history andpast health unremarkable.
Ten-year-old girl assessed because of limitation of neck motion. Born at term to non-consanguineous parents. No history of necktrauma. Family history andpast health unremarkable.
PHYSICAL EXAMINATION
Weight, 28 kg (25th percentile); height, 125 cm (3rd percentile). Short neck, low posterior hairline, and limited range of neck motion. Remainder of examination unremarkable. No Sprengel deformity or scoliosis noted. No heart murmur; normal hearing.
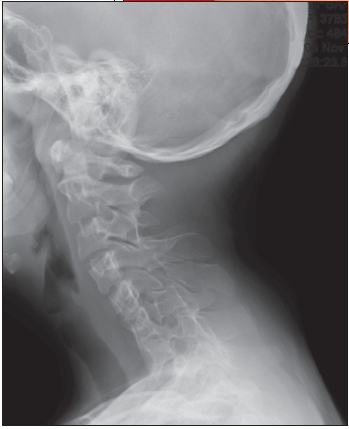
RADIOLOGIC FINDINGS
Radiograph of cervical spine as shown.
WHATS YOUR DIAGNOSIS?
 ETIOLOGY/PATHOGENESIS
ETIOLOGY/PATHOGENESIS
Most cases are sporadic.2 Both autosomal recessive inheritance and autosomal dominant inheritance with variable expression have been described.2-4
Klippel-Feil syndrome results from abnormal embryonic formation of the vertebral mesenchymal anlages and failure of the mesodermal somites to divide during the third to eighth week of gestation.5 The anomaly is most likely caused by disturbed expression or mutation in thePAX 1 gene, which regulates segmentation and resegmentation of the spine.6 The gene has been mapped to chromosome 20p11.2.6
The incidence is estimated at 1:43,000 live births.2,7,8 The female-to-male ratio isapproximately 1.3:1.9
CLINICAL MANIFESTATIONS
 The clinical manifestations of Klippel-Feil syndrome are a short neck, a low posterior hairline, and limitation of head and neck movements. Rotational loss is usually more pronounced than the loss of flexion and extension. The head seems to sit in the thorax. Torticollis or a webbed neck may be present.10 Affected patients might have syskinesia, in which movements in one hand are mirrored in the other.11 The condition is characterized by fusion of 2 or more cervical vertebrae.
The clinical manifestations of Klippel-Feil syndrome are a short neck, a low posterior hairline, and limitation of head and neck movements. Rotational loss is usually more pronounced than the loss of flexion and extension. The head seems to sit in the thorax. Torticollis or a webbed neck may be present.10 Affected patients might have syskinesia, in which movements in one hand are mirrored in the other.11 The condition is characterized by fusion of 2 or more cervical vertebrae.
Three subtypes of Klippel-Feil syndrome are recognized12,13:
• Type 1 presents with massive fusion of the cervical vertebrae and sometimes the upper thoracic vertebrae.
• Type 2 involves fusion at only 1 or 2 cervical intervertebral spaces.
• Type 3 occurs when lower thoracic or lumbar spine anomalies are associated with type 1 or type 2 Klippel-Feil syndrome.
Fusion of the cervical vertebrae might result in hypermobility and instability of the cervical spine at unfused levels, spinal cord compression from disk protrusion, and osteoarthritic changes at a later age.7,10,14 Traumatic tetraplegia has been reported following minor trauma.
Klippel-Feil syndrome is associated with a spectrum of anomalies. Scoliosis occurs in approximately 60% of affected patients; hearing loss in over 50%; genitourinary anomalies in 25% to 35%; rib abnormalities in 33%; Sprengel deformity in 20% to 30%; congenital heart disease in 14% to 29%; and cleft palate in 15%.10,15-17
DIAGNOSTIC STUDIES
Lateral flexion-extension radiographs of the cervical spine confirm the diagnosis and establish the range of motion of each open interspace.2 A lateral radiograph of the skull will demonstrate occipitocervical abnormalities.10 MRI of the cervical cord and craniocervical junction is indicated before any orthopedic procedure and whenever neurologic symptoms or signs are present in the upper extremities.17
Audiology testing is indicated for all affected patients. Kidney and bladder ultrasonography should be performed to screen for urinary anomalies. Echocardiography is indicated when congenital heart disease is suspected.
MANAGEMENT
Treatment is mainly symptomatic. Affected patients should avoid contact sports and any exercise that might exacerbate instability of the cervical spine.