
Hematemesis Caused by Esophageal Duplication

A 17-month-old girl was hospitalized 3 weeks earlier because of gagging and retching emesis that contained blood-streaked mucus. Her symptoms persisted and she was transferred to a tertiary care center for further workup.
The child was born at 35 weeks' gestation after a pregnancy complicated by polyhydramnios. She spent 1 month in the neonatal ICU for feeding difficulties (gurgling sounds during feedings, significant pooling of secretions, and aspiration documented on a video swallow study) and failure to thrive. Results of an upper GI series showed severe gastroesophageal reflux. Findings on an echocardiogram to evaluate ventricular function suggested the presence of a mass within the esophagus compressing the left atrium. An axial CT scan of the chest showed an abnormally thickened, dilated esophagus.
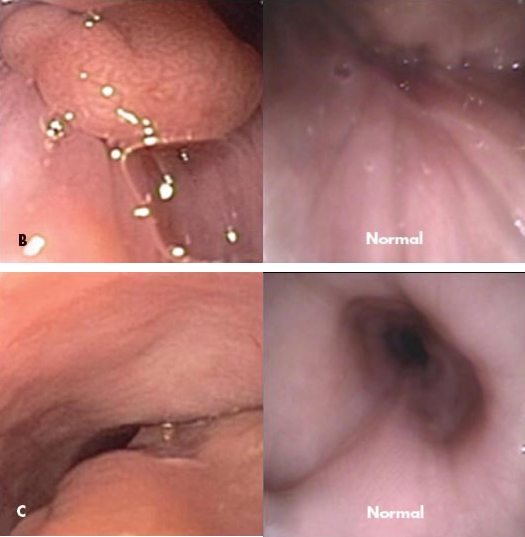
On admission, results of a second GI series revealed a filling defect (A). Upper GI endoscopy revealed a fleshy-appearing, sausageshaped mass (B) that originated above the cricopharyngeus and extended down the whole length of the esophagus, occupying about one-third of the lumen (C). (Views of a normal esophagus at the same anatomic locations are shown for comparison.) The mass surface did not appear vascular or particularly friable. A site of attachment could not be visualized because of the inability to pass the endoscope beyond the mass. Biopsy of the mass showed heterotopic gastric mucosa. Esophageal biopsy revealed mild reflux esophagitis.
The patient underwent surgical resection of a large (5.0 × 2.0 × 2.0-cm), tubular, pedunculated mass. A smooth-surfaced cyst, with a thin (0.1-cm) wall filled with white mucoid fluid was found. Histological examination revealed focal areas of squamous epithelium and predominantly gastric mucosa (both cardiac and antral mucosa) with congestion in the lamina propria (D). Submucosa revealed muscularis mucosa (E) and an area of muscularis propria. These findings were consistent with esophageal duplication.
GI duplications are rare congenital malformations that can be found in any part of the GI tract, the most common location being the small bowel.1 Esophageal duplications account for only 10% to 20% of all GI duplications and affect about 1 of 8000 persons.2 Duplications present in 3 major forms: cysts, diverticula, and tubular malformations.2 Histological features include attachment of the lesion to the GI tract, presence of a muscular layer, and a digestive mucosa.1

Cervical esophageal duplications are rare in children.1,3,4 The finding of gastric heterotopic tissue in this child is unique. Heterotopic gastric mucosa has been associated with other esophageal lesions in adults.5,6
Also referred to as a cervical inlet patch, heterotopic gastric mucosa of the cervical esophagus usually appears as a flat or slightly raised, well-circumscribed, salmoncolored patch.7 Upper GI endoscopy can confirm the diagnosis, although, as shown here, these lesions can be difficult to diagnose preoperatively.