
Hormone-Related Disorders: 2 Types of Abnormal Breast Enlargement

Pubertal Gynecomastia
A 13-year-old boy had bilateral breast enlargement for the past year. There was no associated pain or discharge from the nipples. His past health was unremarkable.
He was not taking any medications. Physical examination findings were otherwise normal. In particular, he had no stigmata of hepatic disease, such as jaundice, palmar erythema, spider angioma, finger clubbing, hepato-spleno-megaly, or ascites. His testicles were of average size.
Pubertal gynecomastia occurs in about 40% of healthy boys typically between 13 and 14 years of age.1,2 The degree of breast development is often so minor that it goes unrecognized unless specifically searched for by palpation. The condition usually resolves over a period of months, but in rare cases it may last several years.1,2
Transient development of breast tissue at the time of puberty is believed to result from a short-lived increase in plasma estrogens (as compared with plasma androgens).3 Both the adrenal gland and the testes are capable of producing estradiol, and there is good evidence for increased peripheral conversion of testosterone to estradiol.3 Also, leptin levels are significantly higher in healthy, nonobese boys with pubertal gynecomastia than in controls.4,5 Presumably, leptin activates estrogen receptors on breast tissue, with resultant gynecomastia.2,4
1. Leung AK. Gynecomastia. Am Fam Physician. 1989;39(4):215-222.
2. Leung AK. Gynecomastia. In: Leung AK, ed. Common Problems in Ambulatory Pediatrics: Symptoms and Signs. New York: Nova Science Publishers, Inc; 2011:263-272.
3. Lawrence SE, Faught KA, Vethamuthu J, Lawson ML. Beneficial effects of raloxifene and tamoxifen in the treatment of pubertal gynecomastia. J Pediatr. 2004;145(1):71-76.
4. Nordt CA, DiVasta AD. Gynecomastia in adolescents. Curr Opin Pediatr. 2008;20(4):375-382.
5. Dundar B, Dundar N, Erci T, et al. Leptin levels in boys with pubertal gynecomastia. J Pediatr Endocrinol Metab. 2005;18(10):929-934.
 Premature Thelarche
Premature Thelarche
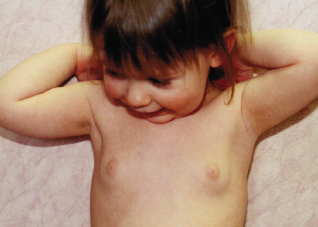
This 2-year-old girl had progressive breast enlargement for the past year. She was born at term to a 23-year-old, gravida 2, para 1 mother, after an uncomplicated pregnancy and normal spontaneous vaginal delivery. Birth weight and length were 3.2 kg and 50 cm, respectively. The infant was exclusively breastfed for the first 6 months. She had been healthy and was not receiving any medications.
The breasts each measured 3 cm in diameter. The vulva, labia majora, labia minora, and vagina were normal.
Premature thelarche denotes isolated breast development before the age of 8 years in girls who do not manifest any other signs of pubertal development.1-3 The condition most often manifests in the first 2 years of life.3 Its occurrence is strongly associated with body mass index standard deviation scores.4 The frequency of premature thelarche is higher among African-American and Mexican-American children.1-3
Premature thelarche may result from an “overactivation” of the hypothalamic-pituitary axis in early childhood secondary to altered sensitivity to steroids of the hypothalamic receptors that control sexual maturation. This causes increased circulating free estradiol, increased sensitivity of breast tissue to estrogens, and increased production of adrenal androgens from the zona reticularis.1-3 The increased adrenal androgens may serve as precursors for the peripheral conversion to estrogens.
Exposure to exogenous estrogens—either indirectly through the breastfeeding mother or directly through estrogen-contaminated foods, drugs, or cosmetics—may cause premature thelarche.1,2 Non-estrogen–containing drugs associated with premature thelarche include spironolactone, digitalis, cimetidine, marijuana, and phenothiazines.1 Although premature thelarche is usually sporadic, a number of familial cases have been reported.1 Some girls with premature thelarche may have an activating mutation in the GNAS1 gene, which codes for a subunit of G-stimulating protein.1,2,5
The enlargement may involve only one breast or one breast more than the other1,2; it is usually not excessive, and no significant changes of the nipples or areolae develop. The breast size may fluctuate cyclically.1,6 Enlarged breast tissue may be tender, but this is usually transient. The vulva, labia majora, labia minora, and vagina remain infantile. No pubic or axillary hair develops. The size of the uterus is consistent with the child’s chronological age. Body habitus is childlike and does not show mature contours. Affected children are of average height and weight. Growth and osseous maturation, the onset of puberty and menarche, and the pattern of adolescent sexual development are all normal.6
With few exceptions, total serum estrone and estradiol concentrations in children with premature thelarche have been shown to be within the normal range for prepubertal girls. Laboratory tests are seldom indicated.
The condition is benign. No therapy is necessary, although repeated parental reassurance is essential. Because breast enlargement may be the first sign of pseudoprecocious or true puberty, a prolonged observation period with monitoring of other pubertal events and linear growth is indicated in all instances.
The prognosis is good. Breast development may regress (32%), persist unchanged (57%), or progress (11%).1,2 The age of onset does not predict whether breast tissue will regress, persist, or progress.7
REFERENCES:
1. Leung AK. Premature thelarche. In: Leung AK, ed. Common Problems in Ambulatory Pediatrics: Symptoms and Signs. New York: Nova Science
Publishers, Inc; 2011:273-276.
2. Leung AK. Premature thelarche. In: Lang F, ed. The Encyclopedia of Molecular Mechanism of Disease. Berlin: Springer-Verlag; 2009:1716-1717.
3. Codner E, Román R. Premature thelarche from phenotype to genotype. Pediatr Endocrinol Rev. 2008;5(3):760-765.
4. Atay Z, Turan S, Guran T, et al. The prevalence and risk factors of premature thelarche and pubarche in 4- to 8-year-old girls. Acta Paediatr. 2012;101(2):e71-e75.
5. Román R, Johnson MC, Codner E, et al. Activating GNAS1 gene mutations in patients with premature thelarche. J Pediatr. 2004;145(2):218-222.
6. Diamantopoulos S, Bao Y. Gynecomastia and premature thelarche: a guide for practitioners. Pediatr Rev. 2007;28(9):e57-e68.
7. de Vries L, Guz-Mark A, Lazar L, et al. Premature thelarche: age at presentation affects clinical course but not clinical characteristics or risk to progress to precocious puberty. J Pediatr. 2010;156(3):466-471.