
Inhalant-Related Acute Eosinophilic Pneumonia in a Young Woman
A 20-year-old young woman presented to the emergency department with a 4-day history of sudden-onset pain and tightness in her lower chest. The pain’s intensity had progressed from 8 to 10 on a 10-point scale and now radiated toward her back. The pain was aggravated with exertion and deep breaths, with no relieving factors present.
She had an associated productive mucoid cough, shortness of breath, and intermittent fever with chills and night sweats. She also reported having had one episode of nonbilious and nonbloody vomiting 4 days before symptom onset. She had no recent history of rash, joint pain, sick contacts, or trauma.
One year ago, the patient had been diagnosed with major depression and anxiety and had been started on trazodone 100 mg daily and citalopram 20 mg daily. She had smoked approximately half a pack of cigarettes per day for the previous 6 months.

Figure 1. Chest radiograph at presentation of a young woman with chest pain and tightness showing bilateral reticulonodular infiltrates, mainly basal in distribution, with blunting of the costophrenic angles.
On physical examination, the patient was in moderate distress, with a temperature of 37.9°C (maximum, 39.0°C), heart rate of 120 beats/min, respiratory rate of 26 breaths/min, blood pressure of 120/48 mm Hg, and oxygen saturation of 93% on room air. Examination findings were unremarkable except for decreased chest expansion related to pain and tenderness over the parasternal region.
Laboratory evaluation revealed a white blood cell count of 17.1 × 103 cells/µL with 90.8% neutrophils, 5% lymphocytes, 3.5% monocytes, 0.6% eosinophils, and 0.1% basophils. Hemoglobin was 9.8 g/dL, hematocrit was 31.1%, and the C-reactive protein level was 13.32 mg/L. Results of a basic metabolic profile were unremarkable except for a bicarbonate level of 20 mEq/L.
Electrocardiogram showed sinus tachycardia. Chest radiographs showed bilateral reticulonodular infiltrates, mainly basal in distribution, with blunting of the costophrenic angles (Figure 1). Computed tomography (CT) angiography with contrast showed bilateral subpleural ground-glass lobular infiltrates with bilateral hilar lymphadenopathy (Figure 2).
With a provisional diagnosis of pneumonia, a regimen of ceftriaxone was started, and oral azithromycin was added to treat atypical organisms, but the patient showed no signs of improvement over 3 days. Laboratory results, including coagulation profile, D-dimer, troponin I, creatine kinase-MB, thyroid-stimulating hormone, free thyroxine, rheumatoid factor, cytoplasmic and perinuclear antineutrophil cytoplasmic antibodies, liver profile, purified protein derivative, and urine toxicology, were unremarkable.
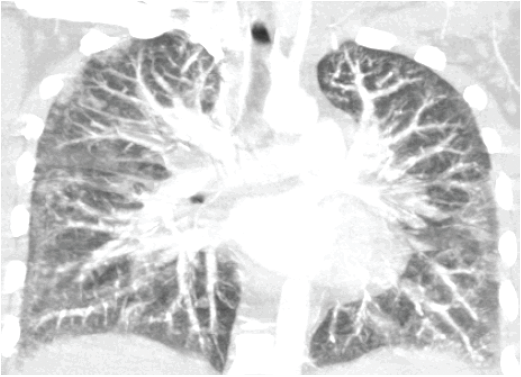
Figure 2. Computed tomography angiography with contrast at initial presentation showed bilateral subpleural ground-glass lobular infiltrates with bilateral hilar lymphadenopathy.
Detailed social history revealed that for the past 6 years, she had been inhaling computer duster (Dust-Off), averaging 10 cans per day. On the third day of admission, bronchoscopy was performed; bronchoalveolar lavage fluid (BALF) analysis revealed a total white cell count of 1556/µL, with 5% polymorphs, 11% lymphocytes, 2% monocytes, and 82% eosinophils. No malignant cells were identified on cytology examination, and the specimen did not grow any bacteria, fungi, or mycobacteria.
The patient was diagnosed with acute eosinophilic pneumonia (AEP) and was started on a 3-week course of oral prednisone 60 mg daily. She showed significant improvement within the first few days of treatment. She stopped inhaling the computer duster but despite counseling continued to smoke about one pack of cigarettes every 3 days.
CT of the chest 2 months later showed resolution of the infiltrates and lymphadenopathy (Figure 3). Corticosteroids were tapered over the next month and then stopped. She showed no recurrence of symptoms during a period of one year.
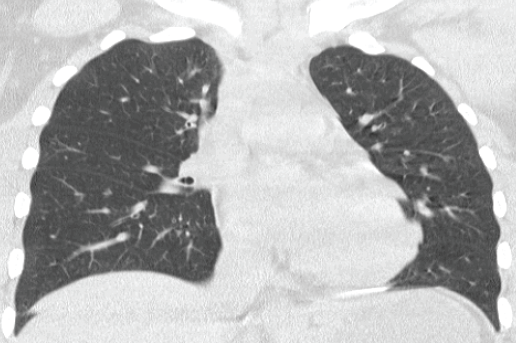
Figure 3. After the young woman’s discontinuation of the inhalant, a high-resolution computed tomography scan of the chest taken 2 months later showed resolution of the subpleural infiltrates and lymphadenopathy.
Discussion
The diagnostic criteria for AEP include the following1:
• Acute onset of any symptoms 7 days or less before presentation
• Fever greater than 37.2°C
• Bilateral infiltrates on chest radiographs
• Severe hypoxemia, arterial partial pressure of oxygen on room air of 60 mm Hg or less, or oxygen saturation on room air of less than 90%, or alveolar–arterial gradient of less than 40 mm Hg
• Lung eosinophilia indicated by BALF differential with 25% or greater eosinophils, or a predominance of eosinophils in open-lung biopsy tissue sample
• No hypersensitivity to medications, no historical or laboratory evidence of infection, and no other known cause of acute eosinophilic lung disease.
Since the first description of AEP in 1989,2,3 many reports have linked this disease with cigarette smoking,4 and this entity has been described in at least one New York City firefighter who was exposed to debris after collapse of the World Trade Center on September 11, 2001.5 To our knowledge, only a single case has been reported so far in which the development of AEP was associated with inhalation abuse of 1,1,1-trichloroethane, a solvent once contained in the fabric protector Scotchgard.6 We report the first case of an adolescent who developed AEP following 6 years of intentionally inhaling Dust-Off computer duster, which contains 1,1-difluoroethane.
More than 22 million Americans aged 12 years and older have used inhalants, and more than 750,000 Americans use inhalants for the first time each year.7 A recent study found that inhalant initiation in the United States peaks at approximately 14 years of age (which is slightly younger than smoking cigarettes or marijuana) and is associated with other recreational drug use.8
Although the exact pathogenesis of AEP remains unclear, Fujimura and colleagues9 showed that in BALF from patients with AEP, the total number of cells, neutrophils, lymphocytes, and eosinophils, along with the ratio of CD4 to CD8 cells, were increased compared with control subjects. An increase in the CD4 to CD8 ratio at onset indicates the induction of helper T cells, which produces interleukin-5 (IL-5). Elevated IL-5 in the lungs may initiate recruitment of eosinophils10 and release chemical mediators from eosinophils,11 which increase the permeability of the vessels. Interestingly, elevated IL-5 in BALF subsided with treatment.12
Similar to cases described in previous reports,2,3,6 our patient showed dramatic improvement with the initiation of a regimen of oral corticosteroids.
As demonstrated by our case, AEP and infectious pneumonia may have a similar clinical presentation, but it is very important to distinguish between the two, because the management differs for these conditions. The diagnosis of AEP usually can be made based on results of a thorough social history, in addition to radiographic evidence and prominent eosinophilia demonstrated in BALF. We believe that 1,1-difluoroethane in computer duster was responsible for the development of AEP in our patient, with cigarette smoking an exacerbating factor.
Given the substantial prevalence of inhalant abuse by adolescents in the United States, pediatricians should be aware of this inhalant-related AEP so that appropriate treatment can be started in a timely manner.
References:
1.Pope-Harman AL, Davis WB, Allen ED, Christoforidis AJ, Allen JN. Acute eosinophilic pneumonia: a summary of 15 cases and review of the literature. Medicine (Baltimore). 1996;75(6):334-342.
2.Badesch DB, King TE Jr, Schwarz MI. Acute eosinophilic pneumonia: a hypersensitivity phenomenon? Am Rev Respir Dis. 1989;139(1): 249-252.
3.Allen JN, Pacht ER, Gadek JE, Davis WB. Acute eosinophilic pneumonia as a reversible cause of noninfectious respiratory failure. N Engl J Med. 1989;321(9):569-574.
4.Uchiyama H, Suda T, Nakamura Y, et al. Alterations in smoking habits are associated with acute eosinophilic pneumonia. Chest. 2008;133(5): 1174-1180.
5.Rom WN, Weiden M, Garcia R, et al. Acute eosinophilic pneumonia in a New York City firefighter exposed to World Trade Center dust. Am J Respir Crit Care Med. 2002;166(6):797-800.
6.Kelly KJ, Ruffing R. Acute eosinophilic pneumonia following intentional inhalation of Scotchguard. Ann Allergy. 1993;71(4):358-361.
7.Howard MO, Bowen SE, Garland EL, Perron BE, Vaughn MG. Inhalant use and inhalant use disorders in the United States. Addict Sci Clin Pract. 2011;6(1):18-31.
8.Nonnemaker JM, Crankshaw EC, Shive DR, Hussin AH, Farrelly MC. Inhalant use initiation among U.S. adolescents: evidence from the National Survey of Parents and Youth using discrete-time survival analysis. Addict Behav. 2011;36(8):878-881.
9.Fujimura M, Yasui M, Shinagawa S, Nomura M, Matsuda T. Bronchoalveolar lavage cell findings in three types of eosinophilic pneumonia: acute, chronic and drug-induced eosinophilic pneumonia. Respir Med. 1998;92(5):743-749.
10.Weller PF. Cytokine regulation of eosinophil function. Clin Immunol Immunopathol. 1992;62(1 pt 2):S55-S59.
11.Tamura N, Agrawal DK, Townley RG. Leukotriene C4 production from human eosinophils in vitro: role of eosinophil chemotactic factors on eosinophil activation. J Immunol. 1998;141(12):4291-4297.
12.Yamaguchi S, Okubo Y, Hossain M, et al. IL-5 predominant in bronchoalveolar lavage fluid and peripheral blood in a patient with acute eosinophilic pneumonia. Intern Med. 1995;34(1):65-68.
Drs Agrawal, Khan, and Dokania are residents in the Department of Pediatrics at John H. Stroger Jr. Hospital of Cook County in Chicago, Illinois. Dr Nickless is a resident in the Department of Family Medicine at Advocate Christ Medical Center in Oak Lawn, Illinois. Dr Bell is the director of inpatient pediatrics and a senior attending physician in the Division of Adolescent and Young Adult Medicine at John H. Stroger Jr. Hospital of Cook County.