
Moving Into 2013: Major Issues Facing Geriatric Care Providers
While 2012 was an active year of change for geriatric care providers, 2013 is expected to be even more turbulent as we get closer to the implementation of major provisions of the Affordable Care Act (ACA), which are scheduled to occur in 2014. As a result, 2013 will be focused on four areas: insurance expansion preparation, reimbursement changes, expansion of accountable outcomes, and increased use of electronic health records (EHRs). To avoid pre-election controversy, regulations in these areas, which were previously released at a trickle, have begun to be released at a record pace. As a result, we are now fully engaged in moving ahead with changes to our healthcare environment.
Because 2013 will be building on 2012 events, it’s important to understand what has already happened to fully appreciate where the healthcare environment is heading. This article provides a review of these events and outlines four major impact areas for geriatric care providers.
2012 Major Events
There were three major healthcare-impacting events in 2012: (1) a major US Supreme Court ruling on the ACA; (2) the Presidential election; and (3) a continued move away from uncoordinated, acute-care–focused, fee-for-service medicine to coordinated care models. The most significant of these events occurred on June 28, 2012, when the Supreme Court ruled that the mandate requiring almost all American citizens to have health insurance starting in 2014 was constitutional.1
Although the Supreme Court did uphold the health insurance mandate, they did force one major change in the implementation of the ACA by stating that the Medicaid expansion would now be a decision for each individual state, rather than a federal mandate. This was the result of the Supreme Court deciding that a state’s total federal dollars could not be tied to a state expanding Medicaid to 133%. The Supreme Court ruled that this was an inappropriate application of federal powers and it severed the Medicaid expansion mandate as a condition of receiving total Medicaid funding. Now states are allowed to opt out of the Medicaid expansion, which could mean that many individuals with lower incomes may not have the expanded healthcare coverage intended for them. As a result, many states are now indicating that they will not expand their Medicaid program as planned by the federal government for 2014.
Also in 2012, the Center for Medicare & Medicaid Innovation continued to expand the number and magnitude of its pilot programs.2 These pilots included accountable care organizations (ACOs), patient-centered medical homes, and hospital readmission reduction programs. An Innovation Center was established under ACA for the purpose of testing, evaluating, and spreading best solutions from innovators around the country to achieve the following objectives:
• Patients always receive the right care, at the right time, and in the right setting.
• Constant improvement of the care delivery system (continuous innovation leads to higher quality care at a lower cost).
• Care is coordinated so that the transitions and communication between healthcare providers and patients are seamless.
• Providers are supported in providing safe, coordinated, seamless care.
• Prevention strategies to keep patients healthy are given as much priority as treating illness.
• Healthcare resources are used efficiently and effectively.
• Ensure rapid spread of the best clinical and delivery system practices.
• A full range of tools—payment, communication, health information technology, training, quality measurement, regulation, and more—are brought together so the system works better for beneficiaries, families, clinicians, and other healthcare providers.
With the help of the Innovation Center, the Centers for Medicare & Medicaid Services (CMS) is working to transform from a claims payer in a fragmented care system into a partner working to achieve better value for our healthcare dollars. The Innovation Center is working to create a healthcare system that provides seamless, coordinated care for beneficiaries, and these activities will continue to expand in 2013. Given that these models are primarily focused on Medicare, its implication for geriatric care providers will be significant. While many of these emerging models will be ACOs, the majority of them will more likely live just outside of the strict Medicare criteria of ACOs and instead be organized as clinically integrated organizations (CIOs). How this terminology is used may be confusing because ACOs are a very specific Medicare program and many integrated healthcare systems are using the term ACO to describe their non-Medicare programs as well. Instead, a more accurate term is CIOs, which describe entities that are clinically integrated providers typically sharing in risk for some accountable outcomes. The bottom line is that an ACO may not be a real ACO, but rather a CIO.
While the healthcare system in 2012 saw continued implementation of the ACA, along with adjustments from the Supreme Court ruling, it also saw the failed initiation of one component of the ACA: the Community Living Assistance Services and Supports Act (CLASS Act).3 This act was to be a national voluntary insurance program for purchasing community living services and supports. The CLASS Act was designed to expand options for people who become functionally disabled and require long-term care services and support. Kathleen Sebelius, the Health and Human Services (HHS) secretary, was expected to define the CLASS benefit by October 2012, with enrollment to begin thereafter; however, the House voted to repeal the CLASS Act in part because Sebelius said she was unable to find a way to make the program financially solvent. As a result, this component of the ACA will not move forward as a program.
In 2012, the application of one specific part of the ACA—the coverage for preventive services—also caused confusion.4 The ACA requires private health insurers to cover recommended preventive services, such as colonoscopies, without any patient cost-sharing. The confusion arises when preventive services turn into treatment. Under ACA, many preventive services are now covered 100%, rather than at the historical 80% for Part B services, which had forced Medicare beneficiaries to pay the uncovered 20%. However, there has been confusion when older adults receive a bill for that 20% for what had been considered a preventive service. This is especially true for colonoscopies that begin as a preventive screening but turn into a treatment when a polypectomy is performed during the procedure. This procedure can turn a screening colonoscopy into a treatment, resulting in a co-payment for patients. It is important that Medicare beneficiaries understand the potential for out-of-pocket payments when undergoing preventive services to avoid surprises.
The Four Points of Impact for 2013
With the continued, albeit modified, rollout of the ACA in 2013, geriatric care providers will feel the impact in four major areas:
• Insurance coverage expansion preparation;
• Reimbursement changes;
• Expansion of accountable outcomes through ACOs and CIOs; and
• Increased use of EHRs.
Although movement in each of these areas has already begun, there will be more significant movement, particularly as we approach 2014.
Insurance Coverage Expansion
While not in effect until 2014, providers will have to start readying themselves for the insurance coverage expansion. Not only will more Americans who are currently uninsured gain insurance, but many who are underinsured will recognize the need to increase their coverage and take the opportunity to do so.
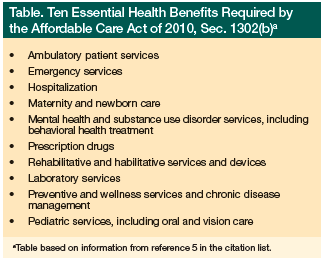 The ACA requires that health insurance plans sold to individuals and small businesses provide a minimum package of services in 10 categories called “essential health benefits” (Table).5 But rather than establishing a national standard for these benefits, the HHS has decided to allow each state to choose from a set of plans to serve as the benchmark plan in their state. Whatever benefits the selected plan covers in the 10 categories will be deemed the essential benefits for all plans in the state.
The ACA requires that health insurance plans sold to individuals and small businesses provide a minimum package of services in 10 categories called “essential health benefits” (Table).5 But rather than establishing a national standard for these benefits, the HHS has decided to allow each state to choose from a set of plans to serve as the benchmark plan in their state. Whatever benefits the selected plan covers in the 10 categories will be deemed the essential benefits for all plans in the state.
In addition to a defined insurance benefit offering, an increased number of individuals will gain insurance through state insurance exchanges,6 federal premium subsidies, and through an expansion of Medicaid. These exchanges are new organizations that will be set up to create a more organized and competitive market for buying health insurance. They will offer a choice of different health plans, certifying participating plans and providing information to help consumers better understand their options.
These state-run exchanges will primarily serve individuals buying insurance on their own and small businesses with up to 100 employees, but states can opt to include larger employers in the future. States are expected to establish exchanges in 2013 and these can be a government agency or a nonprofit organization with the federal government stepping in if a state does not set them up.
For geriatric care providers, while most of our patients will continue to be served by Medicare, some could gain coverage through the state-run insurance exchanges before becoming eligible for Medicare. In addition, some Medicare beneficiaries will gain increased coverage through Medicaid. These changes will force geriatric care providers to be prepared to offer services covered under the essential benefit package and advise patients regarding their new insurance options. Although advising and educating geriatric patients on these new options is not a mandate for geriatric care providers, they are best positioned in many ways to advise and educate their patients on these new options.
Reimbursement Changes
In preparation for an increase in Medicaid beneficiaries, primary care providers will start seeing their reimbursement increase under Medicaid to match the levels being offered through Medicare.7 For many, this could mean a 20% increase when caring for individuals with Medicaid. This increase will remain in effect in 2014, bringing primary care fees for Medicaid, which covers indigent patients, in line with those for Medicare, which insures elders and some disabled patients. Although states and the federal government jointly fund Medicaid, the pay boost would be covered entirely with federal dollars totaling more than $11 billion over the 2 years it would be in effect.
These increases are good news for primary care providers, especially because providers continue to be threatened with two reductions in their reimbursement. First, the Budget Control Act of 20118 imposed caps on discretionary programs to reduce funding by more than $1 trillion during the next 10 years. That act also created a Joint Select Committee on Deficit Reduction to propose legislation to reduce deficits by another $1.2 trillion, and it put in place a sequestration provision to encourage the committee to reach a budget agreement; however, because the Joint Committee was unable to reach a budget agreement, across-the-board payment cuts (and tax increases) took effect in January (“fiscal cliff”). This includes a 2% reduction in the Medicare payment rate and might mean even greater cuts to discretionary federal spending programs, such as Title VII primary care training grants. For now these cuts have been put on a temporary hold, but they continue to loom large.
The second looming cut in physician reimbursement that has been hanging overhead for the last several years is the Sustainable Growth Rate (SGR). Scheduled to impose a 26.5% cut in Medicare reimbursement starting on January 1, 2013, this has once again been delayed. A permanent fix for the SGR has yet to be achieved, and this delay will only increase needed future cuts.9
On top of the proposed 29% reductions, providers are also concerned that additional decreases in reimbursement will come with future financial penalties if they do not successfully participate in multiple Medicare programs, including the e-prescribing program, the EHR meaningful use program, and the Physician Quality Reporting System (PQRS), as well as the value-based modifier. But in addition to sticks, carrots are also being dished out to geriatric care providers.
CMS issued a new policy to pay physicians to coordinate patients’ care in the 30 days following a hospital or skilled nursing facility stay.10 This recognizes the work of community physicians in treating patients following a transition of care and strives to ensure better continuity of care and reduce readmissions. Physicians can bill one of two codes, depending on the complexity of the service provided. The higher-level billing code requires a face-to-face visit with the patient within 1 week of discharge, and this code is expected to provide a reimbursement of $230. The lower-level code, which requires a face-to-face visit within 2 weeks, is expected to provide a reimbursement of $160. These carrots are expected to increase payments to geriatric care providers between 3% and 7%.
Expansion of Accountable Outcomes
The shift from fee-for-service, volume-based reimbursement to pay-for-performance or paying for accountable outcomes means that geriatric care providers will be held accountable for even more outcomes. These outcomes include hospital readmissions, physician quality reporting systems, score on a five-star rating system, and use of e-prescribing and EHRs.
This first year of the Medicare hospital readmission program11 has already estimated it will recoup about $280 million from hospitals that readmit too many patients within 30 days of being treated for a myocardial infarction, heart failure, or pneumonia. This program is expected to be expanded and will impact not only hospitals, but also geriatricians caring for these patients after their discharge. These providers will be held accountable by their hospital partners for implementing systems that reduce hospital readmissions.
This year, Medicare Advantage plans will start to receive bonus payments based on quality ratings. While for several years, CMS has posted quality ratings of Medicare Advantage plans to provide Medicare beneficiaries with additional information about plans offered in their area, Medicare is now using a five-star rating system12 to determine allocation of bonus funds. This focus on Medicare Advantage plan quality measures will force geriatric care providers to deliver on these measures as well.
In addition, CMS will accept PQRS quality measures data extracted from a qualified EHR product for a limited subset of proposed quality measures. Providers who successfully report the PQRS measures are eligible to receive 0.5% of their total estimated Medicare Part B Physician Fee Schedule allowed charges for covered professional services furnished during 2013.
Increased Use of EHRs
In 2013, the availability of funding support for EHRs, which began with the American Recovery and Reinvestment Act (Recovery Act) of 2009,13 will continue to provide for incentive payments for Medicare-eligible professionals who are meaningful users of certified EHR technology. The Recovery Act also authorized spending $27 billion to help providers install and improve EHRs so that they can earn bonus payments from Medicare.
Providers who have yet to implement an EHR system can still do so in 2013. Implementation in 2013 will result in a $15,000 payment from HHS for a total of $39,000 paid over the next 4 years. This represents a $5000 reduction from the maximum $44,000 available to providers who had started their use of EHRs prior to 2013. However, these funds are under attack, as several Congressmen have made an argument to Sebelius, seeking the department to suspend payments to hospitals and physicians practices that switch from paper to EHRs. This is based on their concern that the EHR incentive system “squanders taxpayer dollars and does little, if anything, to improve outcomes for Medicare.” This was presented in a letter to Secretary Sebelius from four Republican House leaders on October 4, 2012.14 In addition, they describe a concern that these EHR systems make it easier for providers to bill inappropriately for more procedures than are needed, as well as more expensive procedures.
Outside of the direct financial incentives and penalties attached to EHRs, these systems may be essential to implementing the use of ICD-10 coding.15 Although the use of ICD-10 had been scheduled for this year, it was delayed until October 1, 2014. ICD-10 implementation will radically change the way coding is currently done and will require a significant effort to implement. For all these reasons, many more providers may start using EHRs this year.
Getting Ready for 2014
Ultimately, much of this year will entail preparation for the future, which starts in 2014 with the health insurance mandate, state insurance exchanges with premium subsidies, millions of additional insured individuals, ICD-10, and implementation of many CMS Innovation Center pilots into national programs. This future promises to mean much more significant changes for geriatric care providers and the older adults they serve. Providers who are able and willing to deliver outcomes for which they will be held accountable will benefit. Of course, this will only come from being prepared to care for an expanding and increasingly complex population of older adults in 2013 and beyond.
The author and series editor report no relevant financial relationships.
References
1. Supreme Court of the United States. October, 2011 Syllabus: National Federation of Independent Business et al. v. Sebelius, Secretary of Health and Human Services, et al. www.supremecourt.gov/opinions/11pdf/11-393c3a2.pdf. Accessed November 13, 2012.
2. About the CMS Innovation Center. Centers for Medicare & Medicaid Services. www.innovations.cms.gov/About/index.html. Accessed November 13, 2012.
3. Title VIII. Community Living Assistance Services and Supports Act (CLASS Act). The White House. www.whitehouse.gov/health-care-meeting/proposal/titleviii. Accessed November 13, 2012.
4. Preventive Care. HealthCare. www.healthcare.gov/law/features/rights/preventive-care/index.html. Updated July 25, 2012. Accessed November 13, 2012.
5. Galewitz P. States Moving Ahead on Defining ‘Essential’ Health Insurance Benefits Under Federal Law. Kaiser Health News. www.kaiserhealthnews.org/stories/2012/october/01/essential-health-insurance-benefits.aspx. Published September 30, 2012. Accessed November 13, 2012.
6. Status of State Health Insurance Exchange Implementation. Center on Budget and Policy Priorities. www.cbpp.org/files/CBPP-Analysis-on-the-Status-of-State-Exchange-Implementation.pdf. Published November 9, 2012. Accessed November 13, 2012.
7. Enhanced Medicaid Reimbursement Rates for Primary Care Services. American College of Physicians. www.acponline.org/advocacy/where_we_stand/access/
internists_guide/v1-enhanced-medicaid-reimbursement-rates.pdf. Published 2011. Accessed November 13, 2012.
8. Senate Bill 365 Amendment. US Government Printing Office. www.gpo.gov/fdsys/pkg/BILLS-112s365eah/pdf/BILLS-112s365eah.pdf. Published August 1, 2011. Accessed November 13, 2012.
9. American Medical Association. Medicare and the Sustainable Growth Rate.
www.ama-assn.org/resources/doc/mss/cola_medicare_pres.pdf. Accessed November 10, 2012.
10. Payments to primary care physicians increase in 2013. Centers for Medicare & Medicaid Services. www.cms.gov/apps/media/press/factsheet.aspCounter=4469&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date. Accessed November 13, 2012.
11. Readmissions Reduction Program. Centers for Medicare & Medicaid Services. www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Updated August 1, 2012. Accessed November 13, 2012.
12. Medicare Health and Drug Plan Quality and Performance Ratings 2013 Part C and Part D Technical Notes. Centers for Medicare & Medicaid Services. www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovGenIn/Downloads/Technical-Notes-2013-.pdf. Updated August 9, 2012. Accessed November 13, 2012.
13. One Hundred Eleventh Congress of the United States of America. US Government Printing Office. www.gpo.gov/fdsys/pkg/BILLS-111hr1enr/pdf/BILLS-111hr1enr.pdf. Published January 6, 2009. Accessed November 13, 2012.
14. The Center for Public Integrity. Top House Republicans demand suspension of electronic medical records program. www.publicintegrity.org/2012/10/05/11189/top-house-republicans-demand-suspension-electronic-medical-records-program. Accessed January 12, 2013.
15. ICD-10. Centers for Medicare & Medicaid Services. www.cms.gov/Medicare/Coding/ICD10/index.html?redirect=/icd10. Updated September 5, 2012.
Accessed November 13, 2012.