
New AGS Guide Offers Useful Information on the Management of Psychotic Disorders and Neuropsychiatric Symptoms of Dementia in Older Adults
The incidence of psychotic disorders and neuropsychiatric symptoms of dementia in later life is substantial. Among those with dementia, an estimated 80% exhibit at least one neuropsychiatric symptom, as do roughly half of those with mild cognitive impairment.1 The timely diagnosis and treatment of psychiatric disorders and neuropsychiatric symptoms in older patients is imperative—but can be challenging due to a number of factors. These include the relatively high prevalence of multimorbidity and polypharmacy in this population and age-related physiological changes that may significantly increase risks of serious medication side effects.
To assist clinicians caring for older patients with these disorders and symptoms, the American Geriatrics Society (AGS) recently published A Guide to the Management of Psychotic Disorders and Neuropsychiatric Symptoms of Dementia in Older Adults, which is accessible via the Web at http://dementia.americangeriatrics.org/GeriPsych_index.php. Based on the seventh edition of the AGS Geriatrics Review Syllabus (GRS) and the 2011 edition of Geriatrics At Your Fingertips (GAYF), this new guide was reviewed by a panel of AGS members from geriatric medicine, geropsychiatry, and geriatric pharmacy, as well as some members of the society’s clinical practice committee and its executive committee.
The new guide is the most recent in a series of high-quality clinical guides the AGS has developed to assist clinicians in the evaluation and management of common problems among older patients and to support evidence-based, high-quality care. Other AGS guides have focused on the diagnosis and treatment of dementia, common immunizations for older adults, and the prescribing of controlled substances in long-term care. (All can be found at www.americangeriatrics.org/health_care_professionals/clinical_practice/featured_programs_products.) The new guide differs in format from previous guides but, like them, provides concise, practical, and well-referenced advice.
The release of the new guide is particularly timely, coming as it does amid continued concerns—among legislators and regulators, as well as clinicians—regarding the overprescribing of antipsychotics—particularly atypical antipsychotics—in long-term care. Psychiatric disorders and their behavioral manifestations and treatment in older adults have recently been a focus of considerable coverage in Clinical Geriatrics.2-4 One of the major lessons learned is that atypical antipsychotic medications—as well as first-generation antipsychotics—can significantly increase risks of death in older patients. Nevertheless, most physicians treating older adults can attest to the value of antipsychotics in selected patients with underlying dementia for behavioral disorders associated with dementia, despite this unapproved use of this class of medications. (Interestingly, recent research suggests that some of these drugs may also be more effective than mood stabilizers in treating mania.5) We are also very aware of the need for careful consideration of the appropriateness of the use of these medications, and of opportunities to reduce dosing, as mandated by the Centers for Medicare & Medicaid Services. There is an excellent summary of studies regarding excess mortality associated with antipsychotic medications in the new AGS guide.
The guide also covers nonpharmacologic management strategies for behavioral disorders associated with dementia. Heightening awareness of the importance of these and of addressing the antecedents and consequences of problem behaviors—rather than simply starting an antipsychotic medication or increasing an existing dose—is essential.
After a brief introduction that links to helpful references, the AGS guide segues to psychotic disorders in later life that, among other things, clearly distinguishes between hallucinations and delusions and includes a flow-chart to aid in the evaluation of older patients with hallucinations, delusions, or both. A helpful section about differential diagnosis follows, highlighting hallmarks of bipolar affective disorder, delirium, dementia, adverse medication effects, major depression, late-life delusional disorder, schizophrenia, seizures, Parkinson’s disease, hypo- and hyperthyroidism, and other contributors to psychosis. The guide includes additional information comparing schizophrenia with late-onset schizophrenia-like conditions. The section on psychotic disorders also offers treatment and management information tailored to the needs of older patients and includes three invaluable tables.
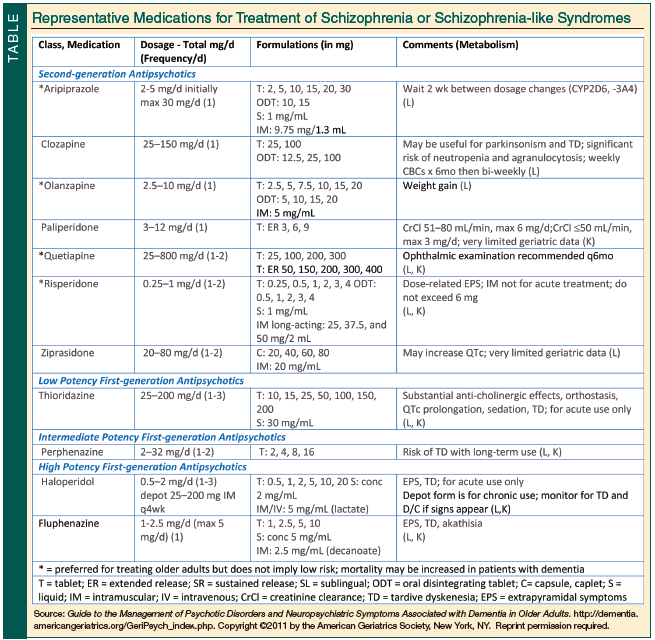
One of these tables, which is reproduced above, lists medications for schizophrenia, as well as dosages, formulations, and related prescribing advice. The other two tables describe adverse events associated with second-generation antipsychotics and summarize treatments for adverse events caused by antipsychotics.
The section of the guide devoted to the management of neuropsychiatric symptoms of dementia describes common symptoms among older adults—including psychotic and depressive symptoms, apathy, manic-like behavioral syndromes, agitation, and aggression—and their hallmarks. It highlights common contributors to transient and long-term neuropsychiatric symptoms and identifies factors that should be taken into account when deciding on treatment. It also includes highly informative tables describing the use of medications for agitation, depressive features, and manic-like features of behavioral disturbances in dementia.
To supplement the information in the guide, I also recommend the AGS GRS and GAYF. And, to help older patients and their caregivers better understand these disorders and symptoms, I recommend the AGS Foundation for Health in Aging “Aging in the Know” Website at www.healthinaging.org/agingintheknow. The site offers easily understandable information about a wide range of later-life health issues, including mental health issues, for patients, family members, caregivers, and others.
Dr. Spivack is Medicare Medical Director, UnitedHealthcare Medicare & Retirement, Westport/Trumbull, CT; Founder, Connecticut Geriatrics Society; Consultant in Geriatric Medicine, Greenwich Hospital, Greenwich, CT, and Stamford Hospital, Stamford, CT.
Send your comments and questions for Dr. Spivack to: medwards@hmpcommunications.com
References
1. Lyketsos CG, Lopez O, Jones B, Fitzpatrick AL, Breitner J, DeKosky S. Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA. 2002;288(12):1475-1483.
2. Tampi RR, Williamson D, Mittal V, McEnerney N, Thomas J, Cash M. Behavioral and psychological symptoms of dementia: part I—epidemiology, neurobiology, heritability, and evaluation. Clinical Geriatrics. 2011;19(5):41-46.
3. Tampi RR, Williamson D, Mittal V, McEnerney N, Thomas J, Cash M. Behavioral and psychological symptoms of dementia: part II—treatment. Clinical Geriatrics. 2011;19(6):31-40.
4. Bharani N. A case of late-onset psychosis. Clinical Geriatrics. 2009;17(3):12-15.
5. Cipriani A, Barbui C, Salanti G, et al. Comparative efficacy and acceptability of antimanic drugs in acute mania: a multiple-treatments meta-analysis. Lancet. 2011; doi:10.1016/S0140-6736(11)60873-8.