
Peer Reviewed
Newborn With Abdominal Mass and Distention
AUTHORS:
Taylor Banks, MD, and John Podraza, MD
Dr Banks is a resident in the National Capital Consortium Pediatric Residency Program in Washington, DC.
Dr Podraza is an assistant professor of pediatrics at the Uniformed Services University of the Health Sciences in Bethesda, Maryland, and a perinatal-neonatal medicine fellow at the National Naval Medical Center in Bethesda.
Dr Banks and Dr Podraza are also lieutenants in the US Navy.
Alexander K. C. Leung, MD—Series Editor
Dr Leung is a clinical associate professor of pediatrics at the University of Calgary and a pediatric consultant at the Alberta Children’s Hospital.
CITATION:
Banks T, Podraza J. What's your diagnosis? Infantile hepatic hemangioendothelioma. Consultant for Pediatricians. 2010;9(5):168-173.
DISCLAIMER: The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the US government.
HISTORY
Baby girl born at 37 weeks' gestation to a gravida 2 para 1, 25-year-old mother by spontaneous vaginal delivery. Apgar scores, 8 at both 1 and 5 minutes. Placenta grossly normal with a 3-vessel cord. Prenatal course uncomplicated. Mother's blood type, A-positive. Results of prenatal testing negative for hepatitis, syphilis, rubella, group B streptococcal disease, and HIV infection. No significant maternal or family history.

PHYSICAL EXAMINATION
Vital signs normal. Birth weight, 3281 g (7.2 lb; 70th percentile); length, 50.5 cm (80th percentile); head circumference, 31 cm (10th percentile). Infant had significant abdominal distention secondary to a palpable smooth mass extending from the right upper quadrant to the right pelvis; liver edge difficult to determine. Mild cutaneous venous congestion over the abdominal wall; no other lesions or rashes. Abdomen firm; no guarding or dullness to percussion. Bowel sounds normal. No splenomegaly or other palpable abdominal masses.

Oropharynx and tongue normal. Lungs clear to auscultation. Heart rate and rhythm regular, with no murmur. Extremities and external female genitalia normal.
LABORATORY FINDINGS
Hemoglobin, 8.6 g/dL; hematocrit, 26.1%; white blood cell count, 31,200/μL; and platelet count, 99,000/μL. Aspartate aminotransferase, 229 U/L; alanine aminotransferase, 39 U/L. Total bilirubin, 5.1 mg/dL, with a direct component of 1.8 mg/dL at 20 hours of life. Prothrombin time of 17.7 seconds, partial thromboplastin time, 36.6 seconds; and international normalized ratio, 1.5.

IMAGING
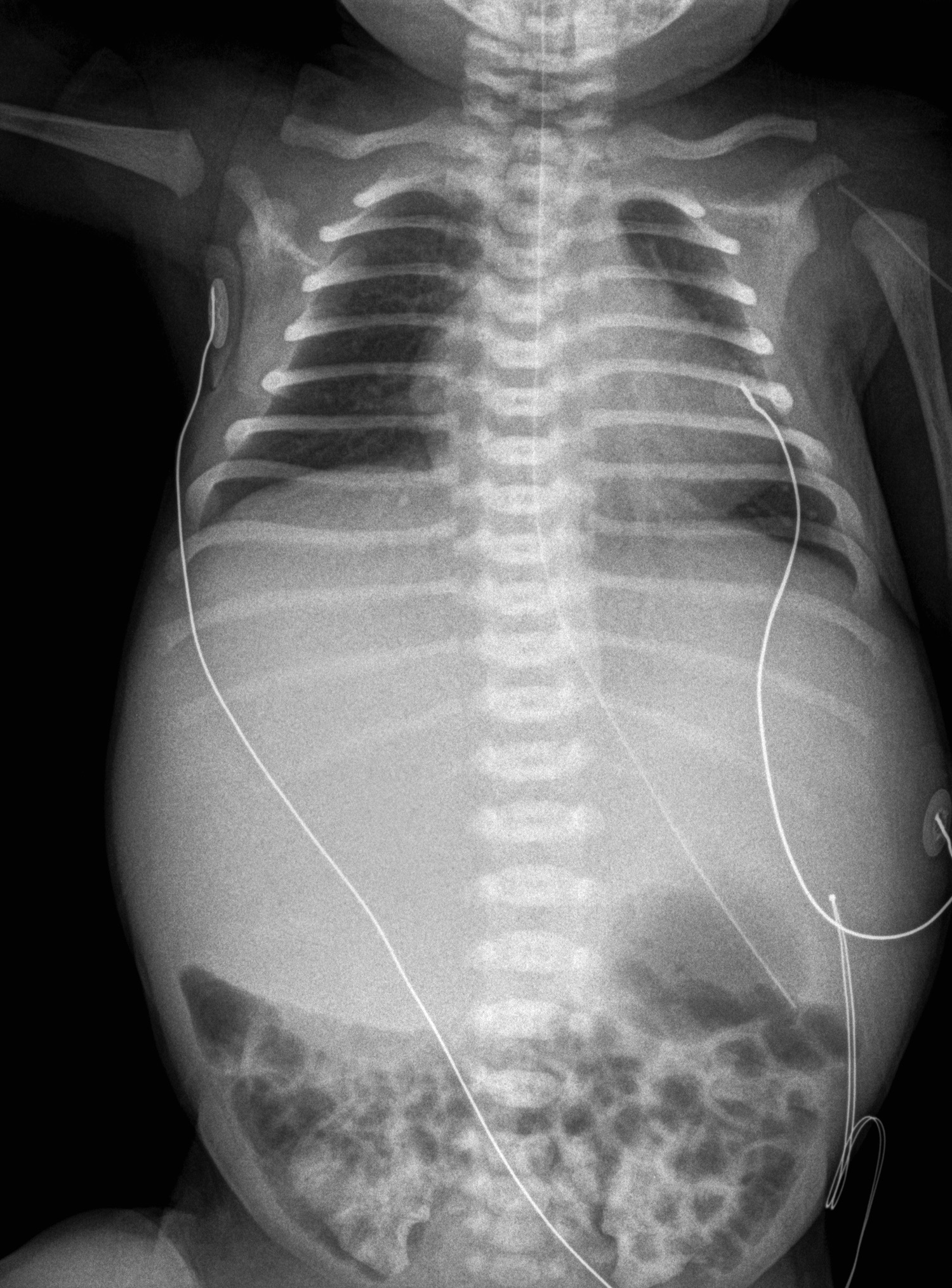
Plain chest radiograph and abdominal CT scan shown.
WHAT'S YOUR DIAGNOSIS?
Answer: Infantile Hepatic Hemangioendothelioma
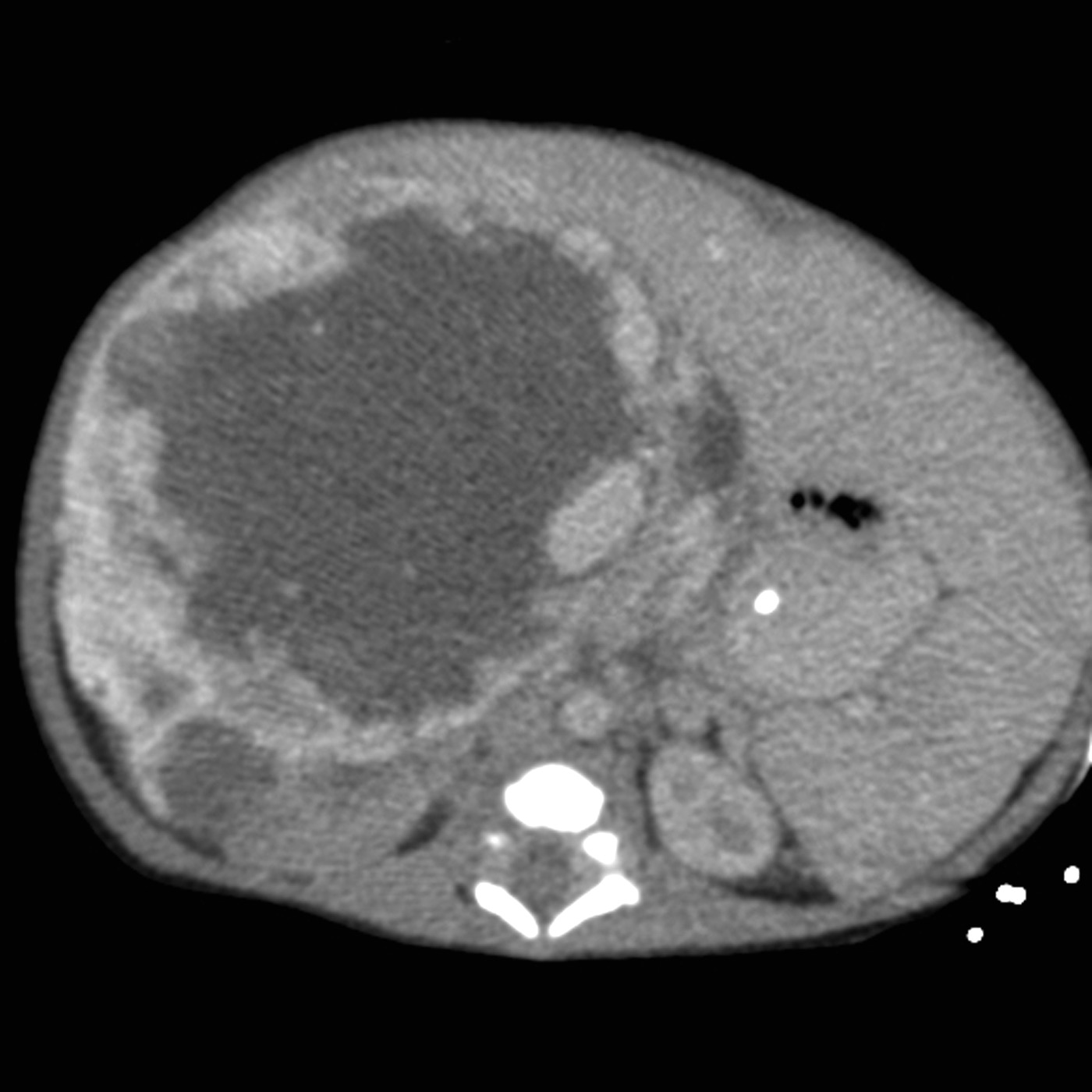
The radiograph showed a large radiopaque mass that encompassed most of the right and left upper quadrants, with multiple loops of bowel displaced into the pelvis, a paucity of bowel gas, and low lung volumes. Abdominal CT revealed a heterogeneous mass with origin in the right lobe of the liver and contact of the left tip of the liver with the spleen (Figure 1). Further evaluation with MRI showed a heterogeneous mass of 8.8 × 6.9 × 8.4 cm with peripheral enhancement and large, nonenhancing areas centrally (Figure 2).
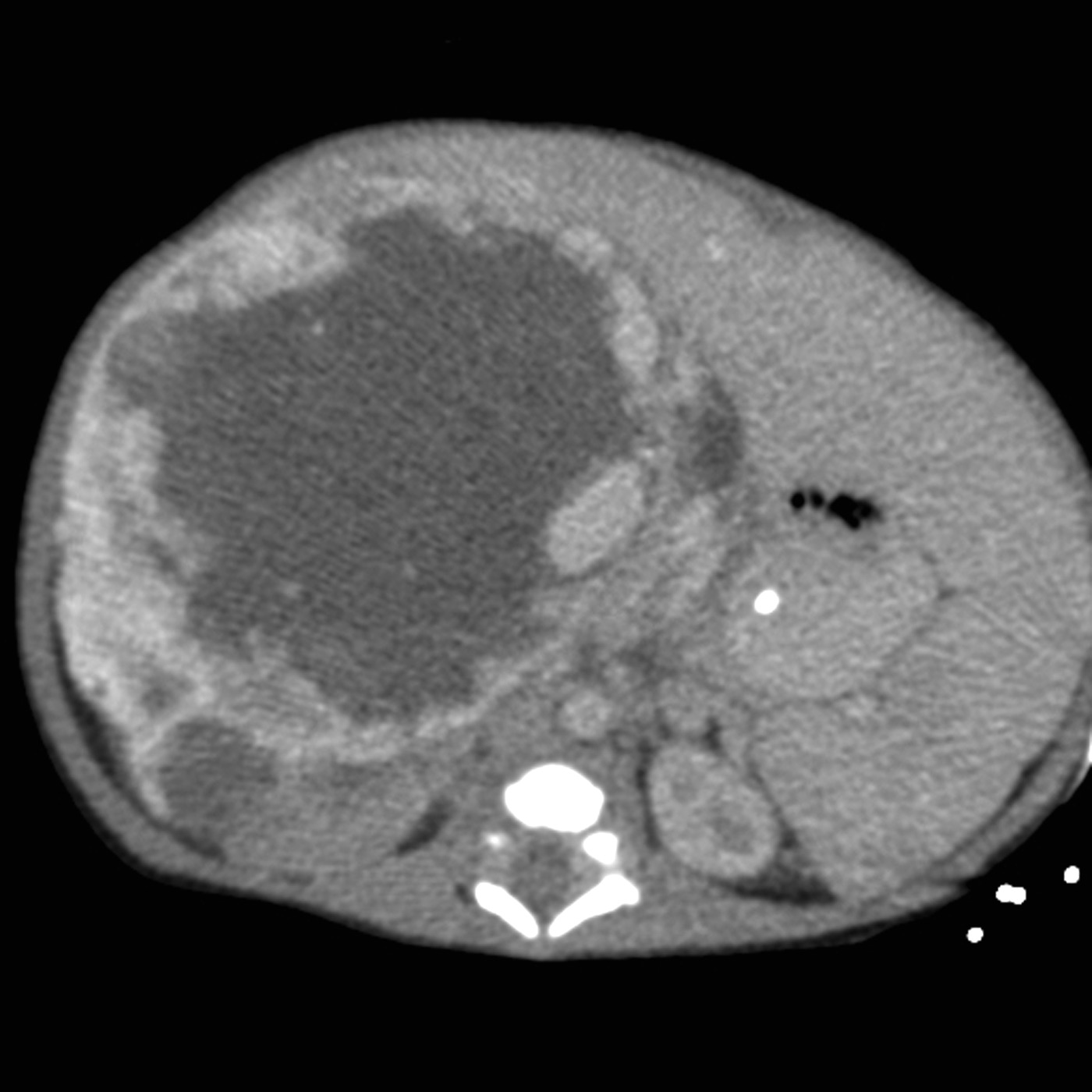
Figure 1 – This abdominal CT slice shows a heterogeneous mass with origin in the right lobe of the liver and contact of the left tip of the liver with the spleen.
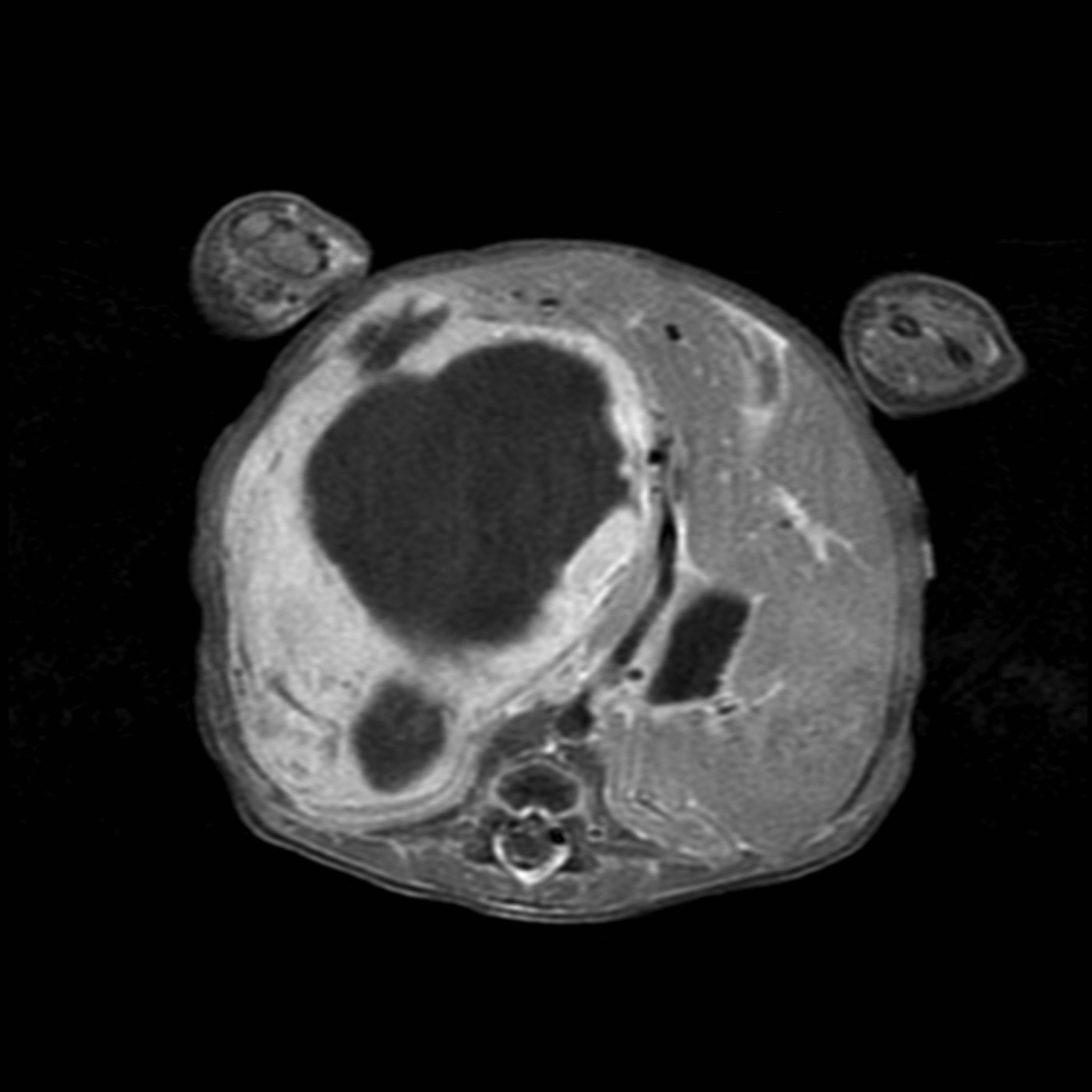
Figure 2 – An MRI scan shows the heterogeneous mass with peripheral enhancement and large, nonenhancing areas centrally.
The radiographic evidence and a decline in the α1-fetoprotein level from 41,142 ng/mL to 25,607 ng/mL over 4 days made hepatoblastoma unlikely. Homovanillic acid and vanillylmandelic acid were not detected in the urine. The adrenal gland was clearly visualized on MRI and CT scans and was ruled out as the lesion's origin.
INCIDENCE AND PATHOPHYSIOLOGY
Infantile hemangioendothelioma is the third most common hepatic tumor in neonates and the most common benign liver tumor in this age-group.1,2 Although 85% of cases manifest by 6 months of age, a neonatal presentation is unusual.3,4 Studies show no clear evidence of genetic transmission3 and no racial predominance in infantile hepatic hemangioendothelioma. However, a 2:1 female predilection has been reported.2
Histopathologically, hepatic hemangioendotheliomas can be separated into 2 types.2,5 Type I consists of multiple vascular channels formed by an immature endothelial lining with stromal separation from bile ductules. Type II is characterized by a more disorganized and hypercellular appearance without the presence of bile ductules. Regardless of type, the vascular nature of the tumor is an important determinant of its appearance on imaging and its clinical sequelae.
Similar to other types of hemangiomas, hemangioendotheliomas have 2 phases of growth: an initial rapid growth phase followed by a period of spontaneous involution. Detection of the mass within the first 6 months of life is attributable to the onset of the tumor's rapid growth phase during this time, although the mass has been detected with fetal ultrasonography.4,6

The initial presentation of a hepatic hemangioendothelioma is variable and usually includes some combination of palpable abdominal mass, hepatomegaly, and abdominal distention.2 Clinical sequelae from these symptoms can be significant. Arteriovenous shunting can cause increased cardiac output and eventual heart failure in up to 50% of patients.2,4 The Kasabach-Merritt phenomenon, characterized by hemolytic anemia, thrombocytopenia, and a consumptive coagulopathy—as seen in this patient—has also been observed.1,2,6,7 Leukocytosis is another common finding. Although absent in this case, cutaneous hemangiomas are present in most patients.3,4
Hepatic hemangioendotheliomas can grow large enough to cause a mass effect within the abdomen. Compression of the liver can result in elevated transaminase levels and obstructive cholestasis.4 Mass effect from the tumor can also impair diaphragmatic excursion and lead to compromised lung expansion and progressively worsening respiratory distress.5 A devastating but fortunately uncommon complication is hemoperitoneum from rupture of the lesion.4
DIFFERENTIAL DIAGNOSIS
Abdominal masses occur in almost 1 of every 1000 live births and have a broad differential diagnosis (Table).5 Identifying the origin of the mass within a tissue or organ system can help narrow the differential. Hepatic masses account for only 5% of all neonatal abdominal masses. The principal lesions in this category are infantile hepatic hemangioendothelioma, cavernous hemangioma, hepatoblastoma, hepatic hamartoma, and choledochal cysts.1,8,9

It is critical to differentiate a benign primary hepatic lesion from hepatoblastoma.2 Hepatoblastoma is the most common primary malignant liver tumor in children and is associated with Beckwith-Wiedemann syndrome, familial adenomatous polyposis, and prematurity. Hepatoblastoma usually presents with greatly elevated levels of α1-fetoprotein. It is often accompanied by thrombocytosis and rarely jaundice.10
Abdominal ultrasonographic or CT findings can often help differentiate hepatic hamartomas and choledochal cysts from hepatic hemangioendotheliomas.11 However, a technetium-excretion scan may be necessary to highlight the biliary tree in the case of choledochal cysts.1

The most important laboratory result to support the diagnosis of hemangioendothelioma is the absence of urine catecholamines. The elevations of α1-fetoprotein levels associated with hemangioendotheliomas are mild compared with those seen in patients with hepatoblastoma.1,12 Histopathological identification via biopsy is often avoided because of the tumor's vascularity.
Imaging that shows a vascular lesion, in a patient with the characteristic clinical manifestations, strongly suggests a diagnosis of infantile hepatic hemangioendothelioma. Ultrasonograms most often show a complex, heterogeneous mass and can show dilation of the hepatic vasculature.2 CT scans show a complex tumor lacking central enhancement secondary to the effects of necrosis, hemorrhage, or fibrosis. Angiography clearly highlights the vascular nature of the lesion and often reveals a dilation of the aorta proximal to the origin of the celiac artery and a striking decrease in diameter distally, indicative of significant shunting.2-4 Calcifications (present in up to 16% of cases) are a nonspecific finding that can also be associated with metastatic neuroblastoma and hepatoblastoma.3,4
MANAGEMENT AND PROGNOSIS
Most lesions spontaneously involute and regress within the first 12 to 18 months of life.2,6 Thus, asymptomatic lesions are generally treated conservatively. Blood products are used to support patients who have severe anemia and/or thrombocytopenia. In patients with cardiac failure, treatment often involves the use of diuretics and digoxin.4
Medical treatments, including corticosteroids and interferon-α-2A, are used in patients with more significant clinical sequelae in an effort to stop further growth and speed regression.6,12,13 Chemotherapy and radiation therapy have also been used to stunt the growth of rapidly enlarging tumors. In severe cases, surgical resection, partial hepatectomy, and embolization of afferent vessels are considered.
The survival rates range from 32% to 75% for symptomatic or complicated cases and are lower for cases in which medical management fails.6,8,14
OUTCOME OF THIS CASE
The infant received a transfusion of both packed red blood cells and platelets. After initial clinical stabilization and investigation of the identity of the tumor, oral prednisone (4 mg/kg divided into 2 daily doses) was started.
At 10 days of life, the patient was discharged with close monitoring by the pediatric hematology/oncology service. She required no further transfusions. At follow-up after about 2 weeks of corticosteroid treatment, an ultrasonogram showed a slight decrease in the lesion size. At age 6 months, the tumor had almost completely regressed, and the patient was doing well.
REFERENCES:
- Chandler JC, Gauderer MW. The neonate with an abdominal mass. Pediatr Clin North Am. 2004;51:979-997, ix.
- Roos JE, Pfiffner R, Stallmach T, et al. Infantile hemangioendothelioma. Radiographics. 2003;23:1649-1655.
- Dachman AH, Lichtenstein JE, Friedman AC, Hartman DS. Infantile hemangioendothelioma of the liver: a radiologic-pathologic–clinical correlation. Am J Roentgenol. 1983;140:1091-1096.
- Keslar PJ, Buck JL, Selby DM. From the archives of the AFIP. Infantile hemangioendothelioma of the liver revisited. Radiographics. 1993;13:657-670.
- Shamaly H, Abu-Nassar Z, Groisman GM, Shamir R. Hepatic hemangioendothelioma: the need for early diagnosis and resection. Isr Med Assoc J. 2006;8:585-586.
- Dabrow S, Neal M, Spoto-Cannons A. Radiological case of the month. Hemangioendothelioma of the liver. Arch Pediatr Adolesc Med. 2000;154:307-308.
- Thompson SM, Dadiz R, Teomete U, et al. Newborn girl with massive hepatomegaly, anemia, and thrombocytopenia. J Pediatr. 2008;152:129-132.
- Schwartz MZ, Shaul DB. Abdominal masses in the newborn. Pediatr Rev. 1989;11:172-179.
- Isaacs H Jr. Fetal and neonatal hepatic tumors. J Pediatr Surg. 2007;42:1797-1803.
- Golden CB, Feusner JH. Malignant abdominal masses in children: quick guide to evaluation and diagnosis. Pediatr Clin North Am. 2002;49:1369-1392, viii.
- Lucaya J, Enriquez G, Amat L, Gonzalez-Rivero MA. Computed tomography of infantile hepatic hemangioendothelioma. Am J Roentgenol. 1985;144:821-826.
- Jothilakshmi K, Matthai J, Paul S, Singal AK. Symptomatic hepatic hemangioendothelioma in a newborn. Indian Pediatr. 2006;43:908-910.
- Woltering MC, Robben S, Egeler RM. Hepatic hemangioendothelioma of infancy: treatment with interferon alpha. J Pediatr Gastroenterol Nutr. 1997;24:348-351.
- Zenge JP, Fenton L, Lovell MA, Grover TR. Case report: infantile hemangioendothelioma. Curr Opin Pediatr. 2002;14:99-102.