
Newborn Nutrition: To Supplement or Not to Supplement?
ABSTRACT: The best practice for newborn nutrition is to offer no food or drink other than human milk, unless medically indicated. Documented inadequate feedings, evidenced by hypoglycemia, significant dehydration, and delayed bowel movements, signal the need for a formal evaluation of a breastfeeding session. Supplementation is started only for the infant whose condition does not improve after a formal evaluation and breastfeeding management. Delayed lactogenesis II cannot be diagnosed until day 3 to 5 after birth or later and must include evidence of inadequate intake. Breastfeeding can be assessed with the LATCH scoring system. Newborns should be consistently feeding well before discharge. Attention must be given to newborns who continue to lose weight after day 7 of life or who are not back to birth weight by 2 weeks of age. The most common reasons for breastfeeding cessation relate to unrealistic maternal expectations. Education is the first and best strategy to promote exclusive breastfeeding.
Since April 2010, the Joint Commission has been tracking rates of exclusive breastfeeding in hospitals in the United States. This new and public way of measuring the quality of newborn care has prompted an increased focus on current policies and procedures regarding the use of supplementation with infant formula within the first few days and weeks after birth.
Under usual circumstances, fewer than 10% of term infants should require supplementation with formula while in the hospital.1 Despite recommendations from the American Academy of Pediatrics (AAP), the CDC, and the World Health Organization (WHO) that infants receive only human milk for the first 6 months, data show that about 75% of mothers initiate breastfeeding, and the rates of exclusive breastfeeding by 3 months and 6 months fall to about 33% and 13%, respectively.1 These rates are even lower in women with low education levels and in non-Hispanic black women.2 In this article, I will review the national recommendations and the rationale behind them, the potential reasons for supplementing with infant formula, and practical ways to promote and support exclusive breastfeeding in the primary care of infants.
BASIS FOR THE CURRENT RECOMMENDATIONS
In general, the use of infant formula should be avoided throughout the first year unless medically indicated. Exclusive breastfeeding will provide the infant with all the calories he or she needs for the first 4 to 6 months and thereafter along with the addition of complementary foods. Feeding human milk to infants is the physiologic norm and gold standard. Human milk is not only nutrition for infants but also a complex, speciesspecific infant support system.3
A review from the Agency for Healthcare Research and Quality on the health outcomes of infants in developed countries revealed that many health advantages, such as reduced risk of acute otitis media andhospitalizations for lower respiratory tract infections, are associated with exclusive breastfeeding.4 In addition, infants who are exclusively breastfed pose less of a financial burden. One recent study concluded that if 90% of US families breastfed exclusively for 6 months, this would save the country $13 billion per year and prevent an excess of 900 deaths.5
Disadvantages of supplementation. Most commercial infant formulas are cow’s milk–based, processed in factories, often concentrated or dehydrated, and packaged and shipped with potential contamination risk. Milk allergy can develop after exposure to as little as 40 mL (1 1/3 oz) of cow’s milk formula.6 These formulas may have additives, such as coconut oil and soybean oil, and unlike human milk, do not contain living, infection-fighting cells. As a result, the gut flora of formula-fed infants has a significantly different microbiological makeup with more anaerobic bacteria and more odor.7
Use of supplementation in the hospital for medical indications or other reasons has been shown to decrease exclusive breastfeeding rates for infants once they are home. Supplemental feedings, regardless of the method, have been found to have a detrimental effect on breastfeeding duration.8 As few as one-third of mothers return to exclusive breastfeeding after supplementation has occurred in the hospital.
 Best practice for newborn nutrition. The AAP has endorsed the WHO and United Nations Children’s Fund “10 Steps to Successful Breastfeeding,” 9 with the exception of step 9 regarding pacifier use (Table 1).10 The AAP supports the use of pacifiers once breastfeeding is well established, because this reduces the risk of sudden infant death syndrome and provides analgesic benefit during painful procedures when breastfeeding cannot be provided.10
Best practice for newborn nutrition. The AAP has endorsed the WHO and United Nations Children’s Fund “10 Steps to Successful Breastfeeding,” 9 with the exception of step 9 regarding pacifier use (Table 1).10 The AAP supports the use of pacifiers once breastfeeding is well established, because this reduces the risk of sudden infant death syndrome and provides analgesic benefit during painful procedures when breastfeeding cannot be provided.10
The 10 Steps are part of the Baby-Friendly Hospital Initiative (BFHI) to promote and suppor t breastfeeding initiation and exclusivity. The goal of the BFHI is to encourage and recognize hospitals and birthing centers that offer an optimal level of care for infant feeding. In 2007, the CDC began surveying all facilities that provide maternity care to measure how closely they follow the 10 Steps.11
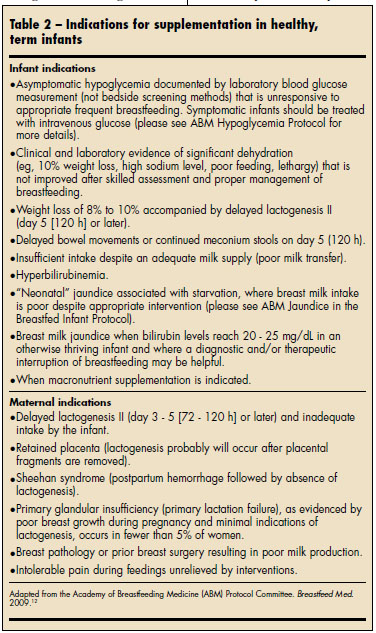
WHEN TO SUPPLEMENT THE HEALTHY, TERM INFANT
When is supplementation medically indicated? An excellent resource for answering this question comes from the Academy of Breastfeeding Medicine (ABM) 2009 protocol (Table 2).12 The ABM makes an important distinction between perceived inadequate feeding and documented inadequate feedings, as evidenced by hypoglycemia, significant dehydration, or delayed bowel movements. The mere presence of any one of these indications for supplementation does not warrant the start of supplementation, but rather a formal evaluation with adequate breastfeeding observation and assistance. Supplementation is started only for the infant whose condition does not improve after a formal evaluation and breastfeeding intervention of the mother-baby dyad.
Perhaps the single-most effective tool in the hospital for determining when to begin supplementation is a formal evaluation of a breastfeeding session. The AAP recommends that a formal evaluation be conducted at least twice daily during the postpartum stay. One objective way to assess breastfeeding is by using the LATCH (Latch, Audible swallowing, Type of nipple, Comfort, Hold) scoring system.13 Similar to the Apgar scoring system, the LATCH system has 5 categories, each of which is assigned a score of 0 to 2.This can be done by the physician caring for the infant, a trained nurse, or a lactation consultant. The goal is for a mother-baby dyad to score 8 of 10 or better for at least 2 consecutive feedings before discharge.
Two events trigger lactogenesis II, the onset of copious milk production: the abrupt fall in progesterone on delivery of the placenta and the prolactin surge that is released every time the baby suckles. Delayed lactogenesis II cannot be diagnosed until day 3 to 5 after birth or later and must include evidence of inadequate intake by the infant.
Other practical indications for evaluating breastfeeding include excessive weight loss (a more than 3% loss on postpartum day 1, more than 7% loss on day 2, or more than 10% loss at any age). Newborns should have at least 1 void for every day they are old until day 4 or 5 and at least 1 stool per day. Also, attention must be given to newborns who continue to lose weight after day 7 of life or who are not back to birth weight by 2 weeks of age. This information distinguishes normal weight loss from severe weight loss and dehdration. For infants with more weight loss than expected, first perform a formal evaluation of the mother-baby dyad with breastfeeding intervention to identify the cause of poor feeding. Then determine whether there is a medical need for supplementation.
What type of supplement to try first? The ABM protocol contains an algorithm for which supplement should be used in order of preference: mother’s own expressed breast milk, pasteurized donor breast milk, protein hydrolysate formula, followed lastly by standard infant formula.
WHY WOMEN CHOOSE TO FORMULA-FEED
To increase the proportion of mothers who achieve the goal of exclusive breastfeeding, we must first consider the reasons why women choose to supplement with infant formula. Medical reasons often cited for supplementation with infant formula include:
- Specific contraindication (eg, maternal HIV infection or illicit substance use).
- Maternal illness or other condition that requires separation from the baby.Nonmedical reasons for supplementation include:
- Lack of education.
- Cultural issues or beliefs.
- Unrealistic expectations.
- Perception that it helps the mother by “letting her rest.”
- Fear that the infant is not “getting enough” breast milk.
- “Why not?” mentality—the belief that feeding with infant formula has no consequences.
HOW TO PROMOTE EXCLUSIVE BREASTFEEDING
Anyone providing frontline care for newborns knows that supplementing without a medical reason is common, and encouraging exclusive breastfeeding is easier said than done. Educating ourselves and new and expectant parents about the recommendation of exclusive breastfeeding and how to achieve this goal should help avoid supplementation most of the time. In doing so, we can help mothers achieve the public health goal of higher rates of breastfeeding initiation, duration, and exclusivity and their own initial desires of breastfeeding.
Education, the first and best strategy. In studies that look at reasons for early breastfeeding cessation (within the first 6 weeks), the most common reasons cited were related to unrealistic maternal expectations, such as perceived inadequate milk supply, frequent feedings, and pain. Often, all parents need is reassurance that their infant is healthy and feeding normally. Tell parents that production depends on supply and demand and that ounces of milk are not expected until day 3 to 5.
For instance, a mother who is unaware that it is normal to make only drops of milk in the first 2 or 3 days may worry, when her baby wants to be at the breast constantly, that she is not producing enough milk. Letting the mother know that every time the baby suckles, her body responds by making more milk—and that skin-to-skin time is a source of comfort for the baby—can allay her fears. Remind overwhelmed parents that in the first week, newborns will probably want to feed every time they are awake. A common misconception among new mothers is that breastfeeding is often painful. The new mother who has pain because of a shallow or ineffective latch may assume that this pain is a normal part of breastfeeding and become very sore and can quickly fall behind in supply. Make sure the mother knows to wait for a wide mouth so that the latch is far beyond the nipple and that the tongue or palate of the baby should not compress or rub the nipple.
Antenatal education has been proven to work. One study noted statistically significant increases in breastfeeding rates at 6 weeks, 3 months, and 6 months postpartum among women who were randomized to view a 20-minute educational video prenatally.14 The US Preventive Services Task Force also recommends interventions to promote and support breastfeeding and that they be given during pregnancy and after birth.15 Skin-to-skin time immediately after birth. The benefits of skin-toskin time have been extensively reviewed16 and are highlighted in the 10 Steps—“help mothers initiate breastfeeding within the first hour after birth” (see Table 1). The AAP and American College of Obstetrics and Gynecology recommend that the infant be placed skin-to-skin with the mother immediately after delivery and that assessments and procedures, such as weighing, bathing, and treating with erythromycin ointment and vitamin K, be delayed until after the first breastfeeding.17 Prompt skin-to-skin time may also help trigger lactogenesis II. The highest prolactin surge occurs with the first feeding and is greater the sooner that feeding is to birth.3
 How recommendations are communicated makes a difference. When discussing feeding plans, rather than simply stating the recommendations, ask questions, such as “What do you like or not like about formula-feeding?” that help you understand the mother’s motivation for breastfeeding. Education can then be tailored to the specific need. Often with simple explanations, many women will choose to try exclusive breastfeeding or at least choose to supplement with expressed breast milk. Women who still want to supplement can be encouraged to use only a small amount of infant formula after attempting breastfeeding. They can then be encouraged to hand express or pump after each formula feeding to enhance milk removal, so that the body receives the signal to make more milk. Mothers may also wish to supplement using an alternate feeding method, such as cup-feeding or syringe- feeding, and avoid use of artificial nipples in the hospital per the WHO guidelines.
How recommendations are communicated makes a difference. When discussing feeding plans, rather than simply stating the recommendations, ask questions, such as “What do you like or not like about formula-feeding?” that help you understand the mother’s motivation for breastfeeding. Education can then be tailored to the specific need. Often with simple explanations, many women will choose to try exclusive breastfeeding or at least choose to supplement with expressed breast milk. Women who still want to supplement can be encouraged to use only a small amount of infant formula after attempting breastfeeding. They can then be encouraged to hand express or pump after each formula feeding to enhance milk removal, so that the body receives the signal to make more milk. Mothers may also wish to supplement using an alternate feeding method, such as cup-feeding or syringe- feeding, and avoid use of artificial nipples in the hospital per the WHO guidelines.
It is important to involve fathers, grandparents, and others who provide the main support for the new mother in these discussions. Their encouragement has been shown to contribute to success. Meeting the mothers and families where they are in their breastfeeding knowledge and providing recommendations and counseling that are tailored to their needs can be helpful. Making recommendations that are informing rather than controlling their feeding decisions will help develop a partnership. As pediatricians, we should not be afraid to recommend breastfeeding or human milk feeding over infant formula in the same way that we feel comfortable counseling new parents about immunizations, smoking cessation, car seats, and safe sleep practices.
Foster a culture of acceptance. Many resources are available to assist in the care of breastfeeding infants (Table 3). If you have not heard of the nonprofit Best for Babes, consider visiting their Web site. Their credo is that all moms deserve to make a truly informed feeding decision and achieve their personal breastfeeding goals without being undermined by cultural and institutional barriers. The Web site contains information designed to help mothers. For providers, it can be a good place to find language that is informing and not controlling for use when talking with colleagues or new or expectant mothers about infant feeding.
REFERENCES:
1. Centers for Disease Control and Prevention. Breastfeeding Report Card—United States, 2010. http://www.cdc.gov/breastfeeding/data/reportcard.htm. Accessed April 7, 2011.
2. Centers for Disease Control and Prevention. Racial and ethnic differences in breastfeeding initiation and duration, by state—national immunization survey, United States, 2004-2008. MMWR. 2010;59:327-334. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5911a2.htm. Accessed April 7, 2011.
3. Lawrence RA, Lawrence RM. Breastfeeding: A Guide for the Medical Profession. 6th ed. Philadelphia: Elsevier Mosby; 2005.
4. Agency for Healthcare Research and Quality. Breastfeeding and maternal and infant health outcomes in developed countries. April 2007. http://www.ahrq.gov/clinic/tp/brfouttp.htm. Accessed April 7 2011.
5. Bartick M, Reinhold A. The burden of suboptimal breastfeeding in the United States: a pediatric cost analysis. Pediatrics. 2010;125:e1048-e1056.
6. Høst A. Importance of the first meal on the development of cow’s milk allergy and intolerance. Allergy Proc. 1991;12:227-232.
7. Mackie RI, Sghir A, Gaskins HR. Developmental microbial ecology of the neonatal gastrointestinal tract. Am J Clin Nutr. 1999;69:1035S-1045S.
8. Howard CR, Howard FM, Lanphear B, et al. Randomized clinical trial of pacifier use and bottlefeeding or cupfeeding and their effect on breastfeeding. Pediatrics. 2003;111:511-518.
9. World Health Organization, United Nations Children’s Fund. Protecting, Promoting and Supporting Breast-feeding: The Special Role of Maternity Services. World Health Organization: 1989. http://whqlibdoc.who.int/publications/9241561300.pdf. Accessed April 12, 2011.
10. American Academy of Pediatrics. http://www.aap.org/breastfeeding/files/pdf/TenStepswosig.pdf. Accessed April 12, 2011.
11. Centers for Disease Control and Prevention. 2007 CDC National Survey of Maternity Practices in Infant Nutrition and Care (mPINC). http://www.cdc.org/mpinc. Accessed April 12, 2011.
12. Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol #3: hospital guidelines for the use of supplementary feedings in the healthy term breastfed neonate, revised 2009. Breastfeed Med. 2009;4:175-182.
13. Jensen D, Wallace S, Kelsay P. LATCH: a breastfeeding charting system and documentation tool. J Obstet Gynecol Neonatal Nurs. 1994;23:27-32.
14. Su LL, Chong YS, Chan YH, et al. Antenatal education and postnatal support strategies for improving rates of exclusive breast feeding: randomised controlled trial. BMJ. 2007;335:596.
15. US Preventive Services Task Force. Primary Care Interventions to Promote Breastfeeding. http://www.uspreventiveservicestaskforce.org/uspstf/uspsbrfd.htm. Accessed April 12, 2011.
16. Moore ER, Anderson GC, Bergman N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2007;18:CD003519.
17. American Academy of Pediatrics and American College of Obstetricians and Gynecologists. Clinical practice guidelines for preconception and perinatal care. In: Guidelines for Perinatal Care. 6th ed. American Academy of Pediatrics; 2007.