
Pediatric Migraine: Clinical Pearls in Diagnosis and Therapy
ABSTRACT: Recurrent headaches are frightening for many parents, who may believe that their child’s headache is caused by a secondary disorder such as a malignancy. Parental concerns may trigger workups that may be unpleasant for the patient and costly for the health care payer. Although underlying malignancy is uncommon, chronic and severe headache episodes in children are disabling and require intervention.
_________________________________________________________________________________________________________________________________
Steven, a 13-year-old boy, experienced his first headache at age 7 years. The frequency, intensity, and duration of his headaches have been increasing over the past 6 months. Steven now experiences 7 to 10 headaches each month that last up to 8 hours. The headaches are associated with mild nausea, light and sound sensitivity, dizziness, fatigue, occasional abdominal discomfort, and difficulty in concentrating. Last year, he had a vomiting episode because of a headache. The pain is usually more prominent in the forehead and does not favor either side of the head. The headaches usually begin in the morning before he leaves for school. As a result, Steven has missed nearly 25% of his school days this semester; his parents are considering home tutoring for "sick children who are unable to attend school."
Steven's mother has treated the headaches with various over-the-counter medications. The pain typically resolves slowly and often recurs the next day. Steven would like to study martial arts but was advised against participation because exercise exacerbates his headaches. Steven's mother suffers from "terrible sinus headaches" that worsen during menstruation. She is very concerned that her son may have a brain tumor or chronic infection.
On presentation, Steven complained of a mild headache and photophobia. His vital signs were stable. Results of the physical and neurologic examination were normal. He had no evidence of meningeal signs.
By age 15 years, 75% of children will have had a significant headache.1 Ten percent of children aged 5 to 15 years and 28% of adolescents aged 15 to 19 years report experiencing migraine headaches.2 Those who experience recurrent headaches are challenged with issues related to school attendance. Within a typical 2-week period in the United States, an estimated 975,000 children reported having a migraine; this resulted in 164,454 missed school days.3 Recurrent headaches also affect a child's participation in social and sporting events, as Steven's case attests. The child's health status can also influence family dynamics.
Here I review the salient details of the history that offer diagnostic clues, discuss the latest diagnostic criteria for migraine in children under 16 years old, describe pediatric migraine precursors, and offer therapeutic recommendations.
CLINICAL EVALUATION
Headache specialists agree that the vast majority of pediatric patients who seek consultation for recurring, disabling headache are migraineurs.3 In a study by Ward and colleagues,4 meningitis, shunt malfunction, and hydrocephalus were diagnosed in only 6% of all emergency department visits prompted by severe headache.All cases of secondary headache disorders in that study were associated with abnormal physical and neurologic findings.4
The diagnosis of pediatric headache disorders is best accomplished by taking a detailed history from the patient and the patient's parents. Key features in children with intracranial disease include altered mental status, abnormal eye movements, optic disc distortion, motor or sensory asymmetry, balance disturbances, and abnormal deep tendon reflexes. Those patients who have abnormalities on examination should undergo additional diagnostic testing.
Focus the history on the patient's headache patterns. Intermittent, disabling headaches in an otherwise healthy and fully functioning person are typical of a primary headache disorder such as migraine. An acute headache that gradually increases in severity over time warrants further investigation to identify possible intracranial disease.
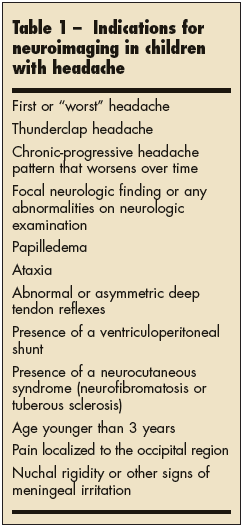 MRI scanning is warranted for those patients who have a chronic-progressive headache pattern or any worrisome features (Table 1). An electroencephalogram is indicated only when the child's headaches are associated with alterations in consciousness or with abnormal involuntary movements.5
MRI scanning is warranted for those patients who have a chronic-progressive headache pattern or any worrisome features (Table 1). An electroencephalogram is indicated only when the child's headaches are associated with alterations in consciousness or with abnormal involuntary movements.5
Lumbar puncture should be performed in patients in whom acute CNS infection is suspected or in those patients with signs of meningeal irritation or lateralizing signs on neurologic examination. Opening and closing pressures should be measured when pseudotumor cerebri, subarachnoid hemorrhage, or meningitis is suspected.
A useful tool for evaluating the impact of migraine on a child's quality of life is the Pediatric Quality of Life Inventory (Peds QL 4.0) generic core scales.6 This age-specific, 23-question document is divided to address 4 age groups and offers questions for parents and children. Evaluated domains include physical, emo- tional, social, and school health.
DIAGNOSIS AND CLASSIFICATION
In 2004, the International Headache Society updated the criteria required for the diagnosis of both migraine with and without aura in children aged 15 years and younger (Table 2).7 The primary difference between adult and pediatric migraines is headache duration, which tends to be shorter in the latter, although they are equally disabling. Like adult migraineurs, pediatric patients experience nausea, photophobia, phonophobia, and difficulty in concentrating. Headaches are exacerbated by exertion and often resolve after vomiting or with sleep. Ninety percent of pediatric migraineurs have at least 1 primary relative who is affected by migraine.3 These children inherit neurologic sensitivity, which makes them easy targets for migraine triggers. Sensitive migraineurs also tend to experience motion sickness and dizziness.
In children, headache pain is likely to be diffuse rather than unilateral. Pain is localized to the frontotemporal regions. Occipital headaches in children, whether unilateral or bilateral, are rare. The child in whom they occur should be evaluated for a structural lesion.3,8 Photophobia or phonophobia occurring in conjunction with nausea or vomiting in children younger than 12 years is most often migraine-related.9 Very young children may become irritable, cry, or cling to a parent because they are sensitive to light and sound during migraine. Unlike adults who have resolution of aura followed by migraine, children may experience an aura and headache simultaneously.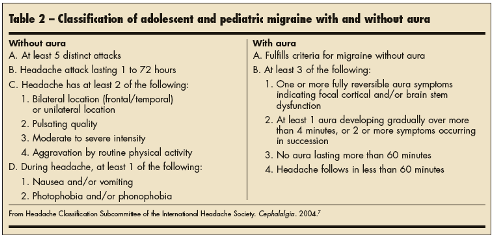
PEDIATRIC MIGRAINE PRECURSORS
Paroxysmal disorders are common in patients who will ultimately be predisposed to migraine. Childhood periodic syndromes--such as cyclic vomiting, abdominal migraine, and benign paroxysmal vertigo--are self-limited and generally do not require an extensive or expensive workup.
Cyclic vomiting syndrome (CVS) in infants and children is characterized by repeated bouts of explosive vomiting, at times to the point that the child becomes dehydrated. The median age of onset is 5 years, but CVS has been observed in infants as young as 6 days. Attacks, which last 1 hour to 5 days, are separated by periods of well-being. Symptoms usually have a rapid onset at night or in the early morning and last 6 to 48 hours. Associated symptoms include abdominal pain (80%), nausea (72%), retching (76%), anorexia (74%), pallor (87%), lethargy (91%), photophobia (32%), phonophobia (28%), and headache (40%). Eighty-two percent of patients with CVS have a family history of migraine.10
The diagnosis of CVS warrants the exclusion of secondary causes of cyclic vomiting in young children, such as intussusception, intracranial hypertension, and inborn errors of metabolism. Prophylactic agents such as cyproheptadine and amitriptyline can be useful in reducing the frequency, severity, and intensity of these disabling attacks.11 Children older than 3 years who have severe and persistent symptoms of CVS associated with recurrent dehydration may be treated with ondansetron 0.15 mg/kg IV q6h.
Abdominal migraine is an idiopathic recurrent disorder characterized by episodic midline abdominal pain. The attacks, which last 1 to 72 hours, are moderate to severe in intensity and are associated with nausea, vomiting, pallor, and anorexia. Between attacks, patients are pain- and symptom-free. The attacks interfere with daily routines and often become sources of concern when a comprehensive diagnostic workup fails to identify a cause. Although patients infrequently experience headache in association with their abdominal discomfort, migraine will most often develop later in life.3
Benign paroxysmal vertigo (BPV)affects younger children (median age, 18 months). During a typical attack, children exhibit acute unsteadiness on their feet, which requires them to grab on to a parent or to a nearby object to avoid falling. Loss of consciousness does not occur, but nystagmus is common. Vomiting may occur and may be vigorous; spells may last several minutes. After each attack, the patient will sleep and return to normal activities on waking.
BPV attacks tend to occur in clusters over several days and then may subside for weeks or months. BPV, like abdominal migraine, is a precursor to adult migraine.12
(Continued on next page)
PATIENT EDUCATION
Treatment of children and adolescents with migraine should focus foremost on behavioral modification and education. Both the patient and the parents should understand the importance of differentiating primary (benign) from secondary (organic) headache disorders. The likelihood of finding a brain tumor in a child with migraine headache who is older than 6 months and whose neurologic function is normal is approximately 0.4%.13 Headaches occur in fewer than 50% of all patients with brain tumors and emerge as the tumor causes an increase in intracranial pressure.14 Concerned parents should be informed that usual symptoms of brain tumors include an altered level of consciousness, ataxia, nausea, vomiting, seizures, or acute onset of weakness in an extremity.
Lifestyle intervention. Successful management of headache disorders requires an integrative approach between pharmacotherapy and behavioral intervention. Parents appreciate physicians who spend time discussing lifestyle changes that can reduce the frequency, intensity, and duration of their child's headaches. Most parents prefer behavioral interventions to pharmacotherapy. Integration of the suggestions in Table 3 can prevent many pediatric migraines.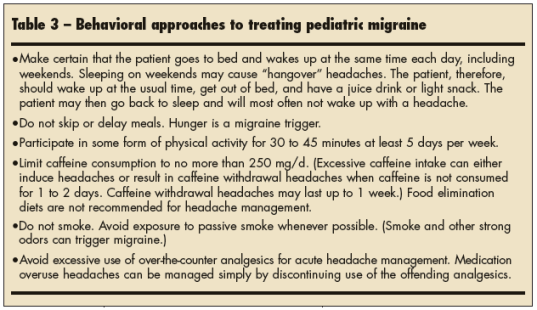
PHARMACOTHERAPY
Reserve preventive and acute medications for patients with frequent and disabling headaches. Acute intervention should begin within 30 minutes; pediatric migraines rapidly reach peak pain intensity within 4 hours and then usually resolve. Medications should be available and accessible both at school and at home. School health services need to be aware of a patient's diagnosis and of the need to rapidly administer the proper medication.
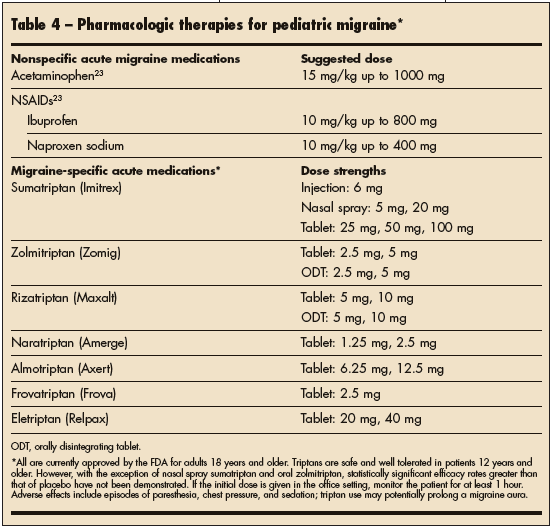
Acute medications.Acute migraine therapies can be classified as migraine-specific or migraine nonspecific (Table 4). Although both types of therapies are effective in pediatric patients, some patients fail to achieve a pain-free state within 2 hours of taking an over-the-counter analgesic. Nevertheless, therapeutic trials of simple analgesics are warranted as first-line acute migraine therapy in treatment-naive pediatric patients. Be on guard for medication overuse headache (MOH).
Analgesics and MOH. Ibuprofen in doses of 7.5 to 10 mg/kg is effective for acute migraine.3 However, using simple analgesics more than twice weekly can lead to MOH.15 Up to 30% of children with chronic daily headache have been shown to use analgesics daily.16
MOH can occur at any age, even in children as young as 2 years. A headache pattern may represent MOH if it typically occurs 15 days or more per month for more than 3 successive months in a patient who frequently uses a simple analgesic. MOH worsens as the patient accelerates analgesic use. Adolescents may complain that the headache awakens them from sleep and is present when they wake up. Immediately on sensing the return of the headache, the patient will take another analgesic or be given additional medication by a parent. Over time, the patient rarely experiences a pain-free interval. Intermittent severe, disabling migraines develop into mild to moderate daily headache.
When analgesics are abruptly discontinued, the headache pattern intensifies once again. However, successful discontinuation of analgesics results in an 80% reduction in headache frequency in most patients.17 As in adults, MOH is associated with the use of simple analgesics; combination drugs that contain butalbital and caffeine; and triptans, opioids, and ergotamines.
Triptans. Several large multicenter double-blind, placebo-controlled trials have shown that triptans are safe and well tolerated in children aged 12 years and older.8 Unfortunately, because of trial design flaws, placebo response rates are high in pediatric migraine studies, which limits our ability to determine the true effectiveness of oral triptans. Open-label trial evidence supports the effectiveness of oral zolmitriptan and subcutaneous sumatriptan in patients 12 to 17 years old.18 Unlike oral sumatriptan, the nasal spray formulation has been found to be safe and effective in acute adolescent migraine.19 Although not approved for use in patients younger than 18 years, triptans should be considered first-line therapy for acute treatment of disabling migraines that are unresponsive to simple analgesics.
A MANAGEMENT GAME PLAN
Always make certain that each patient and his or her family members are completely in agreement on the "game plan" for preventing migraines--as well as how acute medications should be administered. Adherence to the following suggestions improves the overall success of acute migraine management:
•Early intervention (within 30 minutes); this most often results in resolution of pain within 2 hours and less chance of headache recurrence.
•Avoid the frequent use of "backup" or rescue medications.
•Practice and adhere to the lifestyle intervention strategies to reduce neurologic sensitivity.
If you are concerned about possible adverse events associated with triptan use in young children, consider giving the initial dose in the office setting under observation--regardless of whether the patient is symptomatic. Patients who use nasal spray or injections should also practice how to properly use the drugs in the office setting before self-treating their first migraine.
The effectiveness, tolerability, and safety of acute migraine therapy can be evaluated with the help of a headache diary. Patients or their parents are asked to record the date and time of the attack, the trigger, the location of pain, symptoms, severity (on a 10-point severity scale), medication (name, formulation, and dose), time the medication was taken, and the quality of relief (none, moderate, complete) achieved after 2 and 4 hours. Encourage patients or parents to record any other notes about each headache episode that they feel are important to bring to your attention.
PREVENTIVE THERAPY
If frequent or disabling attacks persist despite adequate trials of acute treatments, consider preventive therapy. Choose a regimen based on coexisting conditions and on drug tolerability profiles. Unfortunately, recommendations on preventive medications in children and adolescents are based on information on their use in adults. Data are scant on effectiveness or optimal duration of preventive therapy in pediatric patients.
In children younger than 9 years, cyproheptadine in dosages of 2 to 8 mg/d given at bedtime, or divided and given twice a day, are effective and well tolerated. In older children, adolescents, and adults, adverse effects (such as sedation and weight gain) limit its use. If sleep disturbance is a significant coexisting condition, then cyproheptadine is an appropriate choice. Other preventive agents that can help with sleep are the tricyclic antidepressants amitriptyline and imipramine taken at night in dosages of 10 to 50 mg/d. These agents are also appropriate choices when hyperactivity or enuresis is present. Common side effects are sedation, weight gain, and dry mouth. b-Blockers such as propranolol are often used in dosages of 20 to 80 mg/d that are divided for twice-a-day dosing, although many teenagers do not tolerate the fatigue and exercise intolerance that may occur with this regimen.20
Antiepileptic medications are very effective in preventing migraine attacks. Divalproex sodium is an effective migraine preventive for adults and is often used to treat epilepsy in children and adolescents. However, the adverse-effect profile--weight gain, hair loss, tremor, and risk of birth defects--makes it less desirable as a migraine preventive in this population.21
Topiramate is currently being investigated as a migraine preventive agent in children and adolescents. Dosages for migraine prevention range from 50 to 200 mg/d in single or divided doses.22
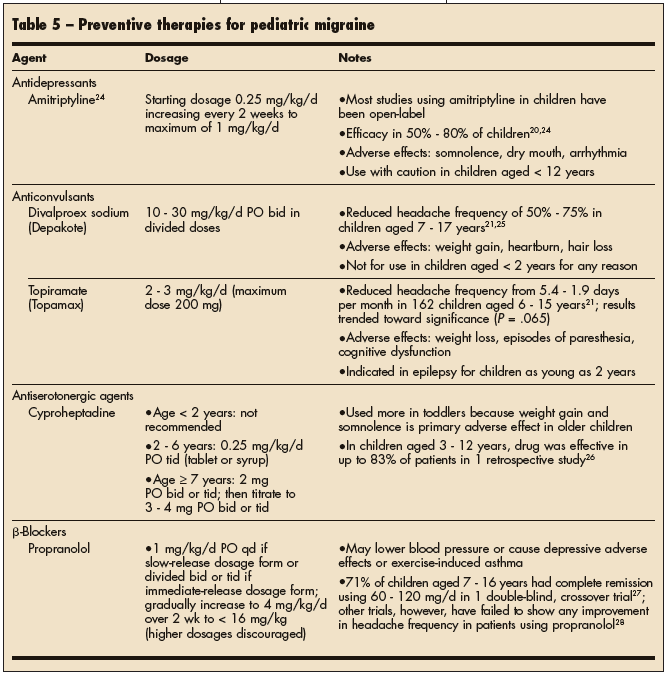 The FDA has not approved any medication for the prevention of migraine in children. The National Headache Consortium Guidelines has suggested that preventive medications should attempt to reduce headache frequency to less than 2 attacks per month for 4 to 6 months. The doses of preventive medications should be titrated slowly to minimize adverse effects. Once sustained relief is achieved, consider weaning the patient from the preventive medications. Preferred preventive therapies for pediatric migraine are summarized in Table 5.
The FDA has not approved any medication for the prevention of migraine in children. The National Headache Consortium Guidelines has suggested that preventive medications should attempt to reduce headache frequency to less than 2 attacks per month for 4 to 6 months. The doses of preventive medications should be titrated slowly to minimize adverse effects. Once sustained relief is achieved, consider weaning the patient from the preventive medications. Preferred preventive therapies for pediatric migraine are summarized in Table 5.
Several herbal remedies (feverfew, riboflavin, coenzyme Q10) have been suggested for use in adults with headaches. However, none of these alternative medicines has been adequately studied for the prevention of headaches in children.