
 THE CASE: A 10-year-old girl has had a worsening rash for 1 week. The mildly pruritic, nontender eruption initially appeared on the child's thighs and then spread to the arms and face. The child's right hand, feet, and ankles have been swollen for the past 4 days, which has made ambulation intermittently painful.
THE CASE: A 10-year-old girl has had a worsening rash for 1 week. The mildly pruritic, nontender eruption initially appeared on the child's thighs and then spread to the arms and face. The child's right hand, feet, and ankles have been swollen for the past 4 days, which has made ambulation intermittently painful.
The patient has no history of recent injury or illness. She denies fever, headache, cough, sore throat, rhinorrhea, chest pain, dyspnea, abdominal pain, dysuria, nausea, vomiting, bloody stools, and bloody or darkened urine. She is not taking any medications.
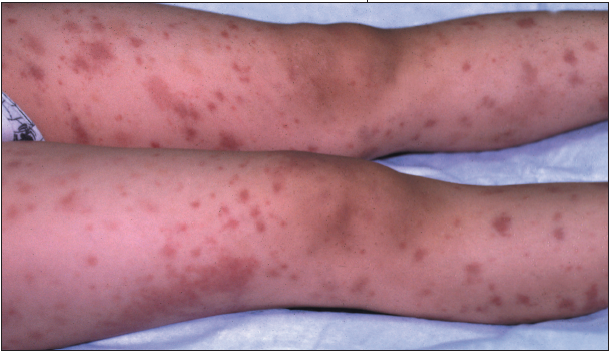
The child, who appears healthy, is in no distress. There are 3- to 6-mm nonblanching erythematous papules and violaceous flat macules on the trunk and upper and lower 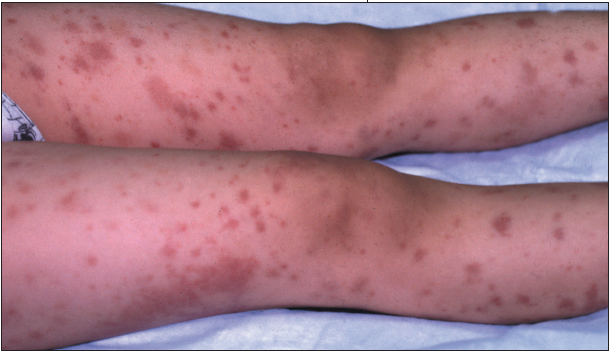 extremities. Dime-sized palpable purpuric lesions are present on both cheeks but are more pronounced on the right.Nonpitting edema of both feet, both ankles, and the right hand is noted. Ankles and feet are neither tender nor erythematous.
extremities. Dime-sized palpable purpuric lesions are present on both cheeks but are more pronounced on the right.Nonpitting edema of both feet, both ankles, and the right hand is noted. Ankles and feet are neither tender nor erythematous.
Which of these conditions best explains the findings?
• Meningococcemia
• Poststreptococcal glomerulonephritis
• Henoch-Schönlein purpura
• Idiopathic thrombocytopenic purpura
(Answer and discussion begin on next page.)
DISCUSSION:This patient has Henoch-Schönlein purpura (HSP), an IgA-mediated leukocytoclastic vasculitis characterized by neutrophil infiltration into the vessel walls of arterioles, capillaries, and postcapillary venules. IgA and small amounts of IgG and C3 are deposited. Clinical manifestations of HSP may be acute--with spontaneous appearance of rash and other symptoms--or gradual; the course is variable.
Half of patients have malaise and low-grade fever, which were not present in this girl. Rash is universal; it is not known whether visceral manifestations occur in the absence of rash. Lesions usually appear initially on the lower extremities and buttocks but may involve the rest of the body. The classic lesion begins as a small wheal or an erythematous maculopapule that initially blanches and later becomes nonblanching, petechial, or purpuric. Purpura, often palpable, evolves from red to purple to rust-colored before fading. Lesions usually appear in crops.
Rare findings include erythema multiforme, erythema nodosum, rheumatoidlike nodules, and angioedema. Arthritis of the large joints develops in two thirds of patients; it causes swelling, tenderness, and pain on motion but usually resolves with no residual deformity or articular damage. Joint effusions, an occasional finding, reveal nonhemorrhagic serous fluid.
GI symptoms occur in more than half of patients and manifest with mild to severe colicky abdominal pain, vomiting, hematemesis, and hematochezia (gross or occult blood). Radiographs may show decreased motility and segmental narrowing as a result of submucosal edema and hemorrhage. Intussusception, obstruction, infarction, and bowel perforation occur rarely.
Renal involvement, which sometimes emerges after other manifestations have resolved, affects 25% to 50% of patients during the acute phase; findings include hematuria and proteinuria. Nephrotic syndrome, moderate azotemia, hypertension, oliguria, and hypertensive encephalopathy occasionally develop. Renal involvement resolves in most patients; however, chronic renal disease develops in some of them.
Other rare complications include CNS involvement, with seizures, paresis, and coma; hepatosplenomegaly; lymphadenopathy; intramuscular hemorrhage; cardiac or eye involvement; and testicular swelling and hemorrhage.
In the absence of significant renal disease, the prognosis for patients with HSP is excellent. The disease is often mild, but subsequent exacerbations and remissions may smolder for 1 year or longer.
This patient was admitted to the pediatric ward for further evaluation, observation, and management. Her pruritus was treated with several doses of diphenhydramine(; it improved overnight, as did the tender edema of the extremities.
Urinalysis showed microscopic hematuria and proteinuria. Results of blood tests revealed anemia, hyponatremia, and hypoalbu- minemia. C3 level was 55 mg/ dL (normal, 82 to 156 g/dL); C4, 7 mg/dL (normal, 12 to 38 mg/dL); and antistreptolysin O (ASO) titer, 656 Todd units/mL (normal, 0 to 130 Todd units/ mL). The erythrocyte sedimentation rate (ESR) was elevated (47 mm/h), and extractable nuclear antibody and antinuclear antibody panels were negative. Results of the complete blood cell count with differential--including the platelet count--were normal. The results of a punch biopsy confirmed the diagnosis.
After overall improvement during her 2-day hospitalization, the patient was discharged with prescriptions for penicillin and diphenhydramine; she was to be monitored by her primary care physician. Two days later, however, she presented with worsening bilateral ankle pain that limited her ability to ambulate. She denied abdominal and chest pain, nausea, vomiting, diarrhea, fever, and chills. She was in moderate distress from pain. There was no nuchal rigidity, tracheal deviation from midline, back tenderness, or fever. Examination showed diffuse palpable purpura, ankle tenderness on motion, and mild edema of both ankles.
 Acetaminophen with codeine( was prescribed, but the pain was relieved only moderately. Radiographs of the ankles showed diffuse soft tissue swelling but no fractures, subluxations, lytic or blastic lesions, or foreign bodies. The patient was admitted to the pediatric ward for pain control; naproxen( was added to the acetaminophen and codeine. A repeated ASO titer showed a modest decrease to 646 Todd units/mL, and the ESR had decreased to 19 mm/h. The C-reactive protein level was elevated at 1.7 mg/dL. The patient was discharged with her pain under control, and she was able to walk with crutches. Her symptoms resolved completely in several weeks.
Acetaminophen with codeine( was prescribed, but the pain was relieved only moderately. Radiographs of the ankles showed diffuse soft tissue swelling but no fractures, subluxations, lytic or blastic lesions, or foreign bodies. The patient was admitted to the pediatric ward for pain control; naproxen( was added to the acetaminophen and codeine. A repeated ASO titer showed a modest decrease to 646 Todd units/mL, and the ESR had decreased to 19 mm/h. The C-reactive protein level was elevated at 1.7 mg/dL. The patient was discharged with her pain under control, and she was able to walk with crutches. Her symptoms resolved completely in several weeks.
Meningococcal disease is caused by Neisseria meningitidis, an encapsulated Gram-negative diplococcus. The disease may manifest invasively or as asymptomatic pharyngeal colonization. Acute infection presents as meningitis, meningitis with meningococcemia, or meningococcemia without meningitis.
Patients with meningococcemia usually appear ill; they display fever, malaise, and progressing symptoms. About 50% to 80% of patients have a petechial rash that begins on the trunk and legs and may involve the ankles, wrists, flanks, and axillae. These lesions rapidly progress to confluent purpura.
Except for the presence of the petechial purpuric rash, our patient displayed most of the signs of poststreptococcal glomerulonephritis (PSGN), including a positive ASO titer, decreased C3 levels, proteinuria, and hematuria. PSGN typically develops following pharyngitis or a skin infection; the latency period is 1 to 2 weeks. Patients have edema and gross hematuria but no fever. However, our patient had no history of pharyngeal or dermatologic symptoms that would suggest streptococcal disease.
Idiopathic thrombocytopenic purpura (ITP) is a hemorrhagic disorder not associated with other causes of thrombocytopenia; the bone marrow of persons with ITP is normal. Patients may display nonpalpable petechiae, purpura, and bleeding from multiple sites, including the oral cavity, GI tract, and CNS. This condition primarily affects children aged 2 to 4 years and adults aged 20 to 50 years. Our patient's age and normal platelet count ruled out ITP.