
 A 9-year-old Hispanic boy, previously in good health, was admitted for evaluation of chronic right cervical adenopathy. The node had been present for about 6 weeks. The patient was initially taken to his primary medical doctor and given dicloxacillin(, but there was no improvement. The patient reported no fever, sore throat, travel history, or animal exposure. He and his parents denied contact with any persons with tuberculosis. During the past year, the patient had undergone extensive dental work for excessive caries.
A 9-year-old Hispanic boy, previously in good health, was admitted for evaluation of chronic right cervical adenopathy. The node had been present for about 6 weeks. The patient was initially taken to his primary medical doctor and given dicloxacillin(, but there was no improvement. The patient reported no fever, sore throat, travel history, or animal exposure. He and his parents denied contact with any persons with tuberculosis. During the past year, the patient had undergone extensive dental work for excessive caries.
On admission, his white blood cell count was 10,000/µL; hemoglobin was 12.4 g/dL; and platelet count was 340,000/µL.3 The sedimentation rate was 57 mm/h. The node was purplish, nontender, and approximately 14 cm in diameter. Results of a PPD skin test were negative.
The node was subsequently incised and drained. Gram stain revealed thin, branching Gram-positive rods. This culture ultimately grew Actinomyces israelii. Therapy was initiated with intravenous penicillin, 2 million units every 6 hours. However, there was little improvement over the ensuing 4 weeks.
Because of lack of improvement, the patient was taken to surgery where a large necrotizing mass was removed. The mass consisted of lymphoid and salivary glandular tissue with chronic granulomatous and suppurative inflammation. The Gram stain again revealed Gram-positive filamentous branching bacteria. Sulfur( granules consistent with actinomycosis were present. The patient tolerated surgery well and is completing oral antibiotic therapy without incident.
 Actinomyces is a Gram-positive anaerobic bacteria that is a normal flora of the oral cavity, write Donald Janner, MD, and Mark Rowe, MD, of Loma Linda University Medical Center, Calif. Clinical infection can occur as cervicofacial, pulmonary, or abdominal disease.1 Cervico- facial actinomycosis occurs in more than half of reported cases and is often preceded by trauma to the oral pharynx or previous dental procedures. Cervicofacial actinomycosis typically presents in 2 distinct forms2:
Actinomyces is a Gram-positive anaerobic bacteria that is a normal flora of the oral cavity, write Donald Janner, MD, and Mark Rowe, MD, of Loma Linda University Medical Center, Calif. Clinical infection can occur as cervicofacial, pulmonary, or abdominal disease.1 Cervico- facial actinomycosis occurs in more than half of reported cases and is often preceded by trauma to the oral pharynx or previous dental procedures. Cervicofacial actinomycosis typically presents in 2 distinct forms2:
• Chronic adenopathy.
• A hard mass over the mandible ("lumpy jaw").
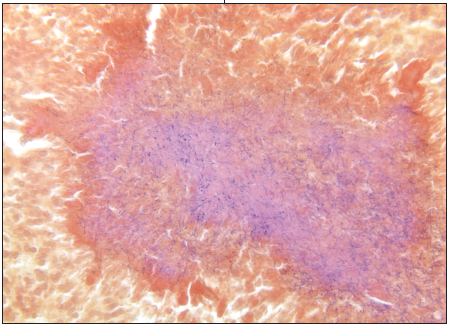
The differential diagnosis of actinomycosis includes mycobacterial disease and catscratch disease. Biopsy is usually needed for definitive diagnosis. Gram stain reveals Gram-positive rods that are thinly branching and weakly acid-fast. Central suppurative necrosis is often seen in biopsy specimens. Infected tissue frequently collects in a purulent material composed of filaments, granulomatous elements, and neutrophils called "sulfur granules," which are pathognomonic of the disease.3
Prolonged antimicrobial therapy has traditionally been the cornerstone of treatment. Patients are often given 4 to 6 weeks of intravenous penicillin followed by 6 to 12 months of oral therapy. While cervicofacial actinomycosis usually responds to antibiotics alone, this is not always guaranteed. In this case, the extent of the disease and the failure of intravenous therapy necessitated surgical excision.