
 A 12-year-old African American boy presented to the emergency department with a painless swelling on the left side of his head that had gradually progressed over a month. There was no history of pain, trauma, or fever. Findings from a review of all other systems were normal.
A 12-year-old African American boy presented to the emergency department with a painless swelling on the left side of his head that had gradually progressed over a month. There was no history of pain, trauma, or fever. Findings from a review of all other systems were normal.
The patient had no significant medical or surgical history. He was well-built and well-nourished. He was afebrile and his vital signs were within normal limits.
The 5-cm swelling on the left frontoparietal region of the scalp was nontender, nonfluctuant, and soft to firm in consistency. There were no signs of inflammation. A circular bony defect approximately 3 cm in diameter was appreciated underneath the swelling.
There was no clinical evidence of similar lesions elsewhere. The patient did not have a rash, lymphadenopathy, hepatosplenomegaly, or bony tenderness.
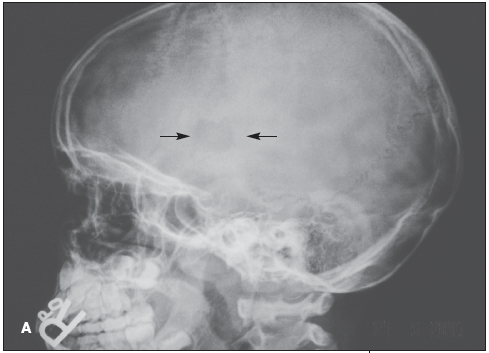
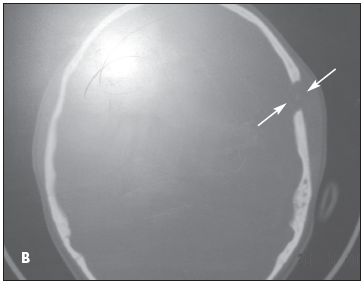
X-ray films of the skull showed a circular defect and an overlying soft tissue swelling (A). CT scans of the head confirmed the solitary bone defect in the skull without any involvement of the brain (B). The complete blood cell count was within normal limits.
The differential diagnosis included chronic osteomyelitis and eosinophilic granuloma (EG).
 A biopsy specimen of the lesion revealed Langerhans cells, which were positive for the CD1a marker. Based on this finding, Manu Kundra, MD, and Helene Tigchelaar, MD, of Children's Hospital of Michigan in Detroit made the diagnosis of EG.
A biopsy specimen of the lesion revealed Langerhans cells, which were positive for the CD1a marker. Based on this finding, Manu Kundra, MD, and Helene Tigchelaar, MD, of Children's Hospital of Michigan in Detroit made the diagnosis of EG.
EG belongs to a group of disorders collectively called childhood histiocytosis. These disorders are all caused by the proliferation and accumulation of cells derived from monocyte-macrophage lineage.1 Based on histopathology, immunology, and electronic microscopic findings, the histiocytoses have been categorized into 3 classes.
Langerhans cell histiocytosis (LCH) belongs to class 1; a number of diseases, including EG, are in this category. LCH most commonly affects the skeletal system--especially in older children, such as this patient. The skull is affected in 80% of cases.1 Patients with EG may have solitary or multiple skull lesions. Symptoms vary depending on the site or extent of involvement or on secondary effects, such as pathologic fractures of the spine leading to cord compression2 or mastoid bone involvement causing otorrhea.3
Therapeutic options include excision of the lesion, corticosteroid injection into the lesion, and low-dose radiation. In this patient's case, local curettage was therapeutic. The child will be followed up every 6 months for 3 years. He is currently asymptomatic. Recurrence is unlikely if no new lesions appear after a year.