
Preventing Recurrent Urinary Tract Infections in a Woman With Dementia
Treatment and prevention of urinary tract infections (UTIs) are important aspects of care for patients with dementia, as UTIs frequently result in superimposed delirium that can accelerate cognitive decline in these patients. When UTIs are recurrent, risk of delirium and subsequent cognitive decline is increased, making this scenario particularly problematic. In addition, management of infections is made more difficult in these patients due to altered voiding patterns and complications from efforts to manage their incontinence (eg, inappropriate use of urinary catheters).1 Numerous studies have examined interventions for preventing recurrent UTIs. Varying results have been reported for cranberry consumption2-4 and for agents such as methenamine5 and antibiotics.6 Probiotics have shown some promise in the treatment of recurrent UTIs.7,8 Among postmenopausal women, intravaginal estrogen cream,9 but not oral estrogen,10 has been shown to reduce the incidence of UTI in those with recurrent infections. We report a case of advanced dementia complicated by recurrent UTIs resulting in delirium that was successfully managed using a systematic hygiene intervention administered by the family caregiver.
Case Presentation
A 72-year-old woman with a 6-year history of probable Alzheimer’s disease showed a decline in cognition as measured by a decrease in Mini-Mental State Examination score, from 23/30 to 0/30 over those 6 years, despite administration of donepezil and memantine. Her medical history included UTIs and degenerative joint disease of the hips, knees, and lumbar spine, which resulted in spinal stenosis. The frequency of her UTIs escalated until she was having two to three per year. These infections were associated with delirium that further accelerated her cognitive decline. The degenerative dementia, in combination with the arthritic changes, impaired her mobility to the point where she required a wheelchair. This combination of factors also began to produce sacral skin breakdown. At that point, her husband decided to use a systematic hygiene intervention to minimize the risk of recurrent UTIs.
A Systematic Hygiene Intervention 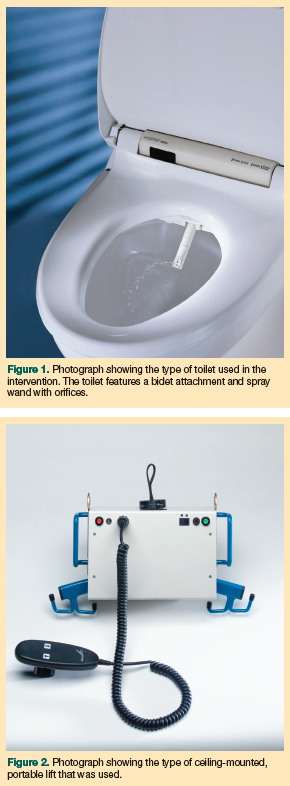 Every morning after breakfast and every evening after dinner the patient is seated on a bidet-type toilet, which features controls for water pressure and temperature and a spray wand with three spray orifices aligned in an anterior-to-posterior direction (Figure 1). Each orifice is capable of spraying in five different directions. The patient is supported on the system by handrails and a stabilizing back sling. When the patient needs to be moved to a vertical orientation for further cleaning, a ceiling-mounted, portable lift machine with a stand-up sling is used to bring her to an upright position (Figure 2). The stand-up sling is used to transfer her to a wheelchair at the end of the procedure.
Every morning after breakfast and every evening after dinner the patient is seated on a bidet-type toilet, which features controls for water pressure and temperature and a spray wand with three spray orifices aligned in an anterior-to-posterior direction (Figure 1). Each orifice is capable of spraying in five different directions. The patient is supported on the system by handrails and a stabilizing back sling. When the patient needs to be moved to a vertical orientation for further cleaning, a ceiling-mounted, portable lift machine with a stand-up sling is used to bring her to an upright position (Figure 2). The stand-up sling is used to transfer her to a wheelchair at the end of the procedure.
For the morning session, the anterior and posterior orifices are used, but the high-pressure third orifice is not. Each of the five spray directions for the anterior spray orifice is activated at maximum pressure for 5 minutes, then each spray direction for the posterior spray orifice is activated for 2.5 minutes, for a total of 37.5 minutes. For the evening session, less waste has typically accumulated since the previous cleaning, so the spray times are 2.5 minutes for the anterior orifice, and 1 minute for the posterior orifice. Altogether, the daily evening cleaning procedure takes a total of 17.5 minutes. During this time, she receives physical therapy exercises for her legs, is bathed, and the upper half of her body is freshly clothed. At the completion of the cleaning procedure, the perineal area is given a final manual cleaning, the patient is dried, and moisturizing cream is applied; an antifungal cream is also used on occasion. This cleaning procedure occurs regardless of whether there has been a bowel movement. Care is taken to never allow a towel or washcloth to touch the genital area after it is used in the perianal area, and towels and washcloths are thoroughly cleaned after a single use. There is also a need for occasional supplementary manual cleaning of the self-cleaning rods that carry the spray heads.
If loose stools have occurred, the shower is turned on and connected to a hose with a hand-operated bidet wand before the patient is seated, then the wand is used to clean the genital area as she is being seated on the toilet seat. The high-pressure orifice on the toilet’s spray wand is used if the patient has diarrhea or if significant fecal material remains after the lower pressure orifices are used; this approach minimizes the abrasion from wiping. The high-pressure orifice is also used when visual inspection shows obvious retained solid fecal matter in the anal canal. Applying high pressure for several minutes in each of the five positions encourages the bowel movement and decreases the chance of soiling between cleaning sessions. Protective undergarments are then applied and her husband finishes clothing the lower half of her body. One caregiver can manage the procedure with the equipment described here.
Case Outcome
With the application of this washing procedure, a bowel movement was induced on 47% of the total days the system was used. If no bowel movement occurred for 3 days, 4 oz of prune juice was given. The juice was needed 1% of the time the system was used. Bowel movements into the protective undergarment outside the setting of the washing procedure have been rare, typically occurring when the patient had diarrhea. The lower frequency of stool in the undergarments resulted in a markedly reduced exposure of the urethral area to fecal material, and the patient had no further problems with skin breakdowns. The patient and her caregiver have used this system for the past 5 years, and the patient had a total of only three UTIs during that time span. The patient exhibited no other health issues during this period, and her husband and healthcare providers did not observe further cognitive decline.
Discussion
Recurrent UTIs can be problematic in elderly women, particularly when complicated by cognitive impairment, incontinence, and loss of ambulatory ability.11 Current treatment options for preventing recurrent UTIs are characterized by equivocal effectiveness and some element of risk. We report a case of an intervention directed at systematically optimizing hygiene to prevent recurrent UTIs.
Hygiene is often mentioned as an important aspect of intervention in elderly women with cognitive impairment, but is seldom studied.11,12 Some studies suggest a role for hygiene in young healthy women. During pregnancy, wiping back to front after urination has been reported to be associated with a greater risk of UTIs than wiping front to back.13 Postcoital washing and voiding has also been reported as being associated with a decreased risk of UTI in young healthy women.14 Despite these two reports, however, most such isolated hygiene measures have not been associated with decreasing recurrent UTIs in larger studies.15-17 One additional study reported that the risk of UTIs among young healthy women was increased during military deployment in conditions where resources for self-care were limited or unavailable,18 which also implies that poor hygiene may be responsible.
The success of the intervention for the case patient raises the question of whether more aggressive hygiene interventions might be beneficial for other elderly patients, including those with dementia and impaired ambulation. The procedure may be limited to patients who do not have major behavioral disturbances and can tolerate it. There is also an initial cost (approximately $7200) associated with setting up such a hygiene procedure, but this cost may be offset by a decrease in subsequent healthcare burdens, including decreased hospitalization for delirium related to recurrent UTIs and delayed placement in an extended care facility.
The use of water as the primary cleansing agent was supported by data from a small study in 2008 that showed no greater risk of UTI when cleansing before catheterization was done with sterile water compared with antiseptic cleansing.19 In the procedure described here in detail, warm water under pressure also appears to relax the anal sphincter. This allows evacuation of stool during cleansing, rather than into protective undergarments later, thereby reducing exposure of the urethra to fecal material over time. Further investigation of more aggressive hygiene measures, such as the one described in this case report, may be worth exploration as low-risk interventions to prevent UTIs in women with dementia.
Conclusion
Recurrent UTIs are problematic for patients with advanced dementia, as they can lead to delirium and accelerate cognitive decline. Various methods have been used to prevent these recurrent infections, with equivocal effectiveness and some element of risk. Our case patient had advanced dementia and recurrent UTIs that resulted in delirium. To prevent her UTIs and their complications, her husband devised a systematic hygiene intervention that consisted of twice-daily comprehensive perineal cleanings, designed to minimize urethral exposure to fecal material. After initiation, the frequency of her UTIs decreased from three per year to a total of three over a 5-year period. The success of the intervention raises the question of whether such an intervention might be beneficial for other patients with dementia. The potential efficacy of this measure, as well as the potential reduction of healthcare costs due to hospitalization from delirium associated with UTIs, may warrant further investigation.
Dr. Beversdorf is the William and Nancy Thompson Endowed Chair in Radiology, Thompson Center for Autism and Neurodevelopmental Disorders, and Associate Professor, Departments of Radiology, Neurology, and Psychological Sciences; Dr. Foster is Assistant Professor of Clinical Obstetrics and Gynecology; and Dr. Tatum is Assistant Professor of Clinical Family and Community Medicine, University of Missouri, Columbia, MO. Mr. Galloway is a retired actuary living in Columbus, OH.
Dr. Tatum received speaker honoraria from the California Academy of Family Physicians to develop a curriculum to teach palliative care to family medicine doctors. The other authors report no relevant financial relationships.
References
1. MacMillan RD. Complicated urinary tract infections in patients with voiding dysfunction. Can J Urol. 2001;8(suppl 1):13-17.
2. Cimolai N, Cimolai T. The cranberry and the urinary tract. Eur J Clin Microbiol Infect Dis. 2007;26(11):767-776.
3. Guay DR. Cranberry and urinary tract infections. Drugs. 2009;69(7):775-807.
4. Jepson RG, Craig JC. Cranberries for preventing urinary tract infections.
Cochrane Database Syst Rev. 2008;1:CD001321.
5. Lee BB, Simpson JM, Craig JC, Bhuta T. Methenamine hippurate for preventing urinary tract infections. Cochrane Database Syst Rev. 2007;4:CD003265.
6. Masson P, Matheson S, Webster AC, Craig JC. Meta-analysis in prevention and treatment of urinary tract infections. Infect Dis Clin North Am. 2009;23(2):335-385.
7. Goldin BR, Gorbach SL. Clinical indications for probiotics: an overview. Clin Infect Dis. 2008;46(suppl 2):S96-S100, discussion S144-S151.
8. Reid G, Dols J, Miller W. Targeting the vaginal microbiota with probiotics as a means to counteract infections. Curr Opin Clin Nutr Metab Care. 2009;12(6):583-587.
9. Raz R, Stamm WE. A controlled trial of intravaginal estradiol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329(11):
753-756.
10. Stamm WE, Raz R. Factors contributing to susceptibility of postmenopausal women to recurrent urinary tract infections. Clin Infect Dis. 1999;28(4):723-725.
11. Nygaard I, Johnson JM. Urinary tract infections in elderly women. Am Fam Physician. 1996;53(1):175-182.
12. Breitenbucher RB. UTI: managing the most common nursing home infection. Geriatrics. 1990;45(5):68-70, 75.
13. Persad S, Watermeyer S, Griffiths A, Cherian B, Evans J. Association between urinary tract infection and postmicturition wiping habit. Acta Obstet Gynecol Scan. 2006;85(11):1395-1396.
14. Amiri FN, Rooshan MH, Ahmady MH, Soliamani MJ. Hygiene practices and sexual activity associated with urinary tract infection in pregnant women. East Mediterr Health J. 2009;15(1):104-110.
15. Hooton TM, Scholes D, Hughes JP, et al. A prospective study of risk factors for symptomatic urinary tract infection in young women. N Engl J Med. 1996;335(7):468-474.
16. Scholes D, Hooton TM, Roberts PL, Stapleton AE, Gupta K, Stamm WE. Risk factors for recurrent urinary tract infection in young women. J Infect Dis. 2000;
182(4):1177-1182.
17. Foster RT Sr. Uncomplicated urinary tract infections in women. Obstet Gynecol Clin North Am. 2008;35(2):235-248, viii.
18. Lowe NK, Ryan-Wagner NA. Military women’s risk factors for and symptoms of genitourinary infections during deployment. Mil Med. 2003;168(7):569-574.
19. Cheung K, Leung P, Wong YC, et al. Water versus antiseptic periurethral cleansing before catheterization among home care patients: a randomized controlled trial. Am J Infect Control. 2008;36(5):375-380.