
Rare Tattoo Complication: Haemophilus influenzae Sepsis in a Teenager
A previously healthy, HIV-negative, fully immunized 18-year-old young adult presented with a 3-day history of pain in his right shoulder and upper chest, which had progressed after 24 hours to swelling and pain in the left knee and leg. He also had an associated fever of 38.9°C of 2 days’ duration.
A large conventional tattoo had been placed on the teenager’s upper chest 2 weeks prior to the onset of illness. The tattoo had healed appropriately within a week of application.

Figure 1. Swelling and tenderness were noted over the right sternoclavicular joint 2 weeks after the application of a tattoo at the site.
Physical examination revealed a well-built, febrile, sick-looking young adult in significant distress as a result of severe pain in his upper chest and left leg. He had a temperature of 40.0°C, a heart rate of 106 beats/min, and blood pressure of 131/86 mm Hg.
Swelling and tenderness were noted over the right sternoclavicular joint (Figure 1). He had decreased range of motion (ROM) in the right shoulder. Also noted were swelling and erythema with warmth and tenderness of the left knee, extending to the calf (Figure 2), which was associated with decreased ROM in the left knee. The neurovascular bundle in the left foot was intact. The tattooed skin of the adolescent’s upper chest looked normal.
His white blood cell (WBC) count was 12.2 × 109/L with 81% neutrophils. The C-reactive protein level was 359 mg/L. The creatinine kinase level was normal.

Figure 2. Swelling with erythema, warmth, and tenderness of the left knee, extending to the calf, were noted on physical examination.
Imaging Studies
Results of chest radiography and Doppler ultrasonography of the left lower extremity and the right upper extremity were normal. A computed tomography scan with contrast showed intramuscular swelling in the left calf with complex, multiloculated, intermuscular fluid collections and intact fascial planes (Figure 3). Magnetic resonance imaging showed focal marrow edema on either side of the right sternoclavicular joint space and moderate joint effusion with intra-articular debris in the left knee.
Joint Aspiration
Arthocentesis of the left knee, performed after 2 doses of ceftriaxone, yielded 40 mL of serosanguineous fluid that had a WBC count of 8.4 × 109/L with 91% neutrophils. Surgical drainage of the left calf revealed multiple pockets of pus with foul-smelling sanguinopurulent fluid. He was treated empirically with intravenous vancomycin, ceftriaxone, and clindamycin.
Synovial fluid culture and all wound cultures were negative, but blood culture grew a pansensitive, nontypeable Haemophilus influenzae strain of biotype I. The antibiotic treatment regimen was changed to intravenous cefuroxime. Wound packing was removed 4 days later. The fever resolved and symptoms improved after the first 2 hospital days.
The patient was discharged on day 5 with instructions to complete 4 weeks of treatment with oral cefpodoxime.
At a follow-up visit 1 week later, the patient was ambulating, pain-free, and had healthy granulation tissue of the left calf wound.
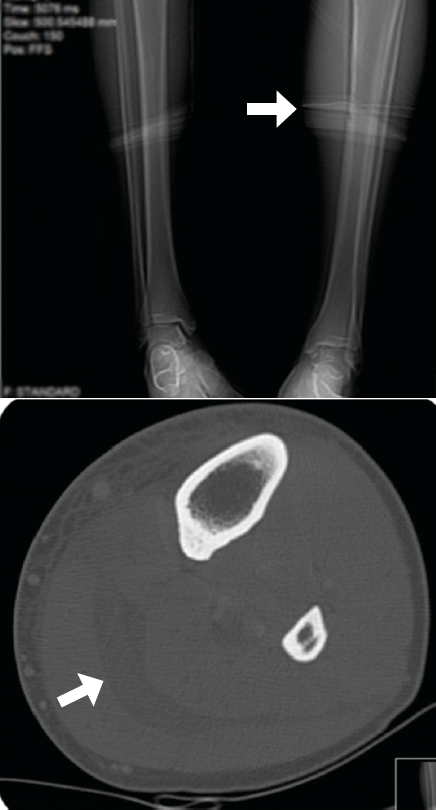
Figure 3. Computed tomography with contrast of the left leg showed complex, multiloculated, intermuscular fluid collections and some intramuscular swelling in the left calf.
Tattoos and Complications
Tattooing has been practiced for thousands of years and has even been noted in several Egyptian mummies.1 Today, 10% to 16% of U.S. adolescents have permanent tattoos, and one-third to one-half of them have one or more piercings other than of the earlobe.2
Complications of tattooing include aseptic inflammation, allergic reactions, pyogenic infections (eg, impetigo, furunculosis, cellulitis), and nonpyogenic infections (eg, syphilis, leprosy, mycobacteria, viral hepatitis).
In the preantibiotic era, bacterial complications of tattooing sometimes were severe or even fatal.3
Today, sepsis after tattooing is extremely rare. It most often is reported after Polynesian or other tribal tattooing with the use of nonconventional needles.4 The causative organisms in these few reports were Pseudomonas aeruginosa, Staphylococcus aureus, and Streptococcus pyogenes.5 To the best of our knowledge, our patient is the first reported case of H influenzae as a cause of sepsis after tattooing.
influenzal Bacteremia
Before the introduction of the flu vaccine, H influenzae serotype b (Hib) was the leading cause of bacterial meningitis and other life-threatening invasive bacterial diseases among children younger than 5 years of age in the United States.
In the post-Hib vaccine era, the majority of invasive H influenzae infections among all age groups in the United States are caused by nontypeable H influenzae,6 with biotype I being one of the emerging strains.7 In fact, in 2006 in the United States, 63% of cases of invasive H influenzae disease in children, and 65% of cases in adults, were caused by nontypeable strains.8
H influenzae bacteremia most frequently occurs in individuals with an underlying predisposing condition such as HIV infection, diabetes mellitus, cancer, or immunodeficiency.9 Our patient had neither an underlying condition nor a local infection immediately after having received a tattoo.
The development of sepsis due to soft tissue focus in association with local deep venous thrombosis is well known, especially in association with S aureus.10
It is likely that the primary H influenzae replication site in our patient was a local microthrombus that was not identified with the use of Doppler ultrasonography. This would explain the multifocal distal septic emboli. The initial decision to administer empiric broad-spectrum antibiotics proved a prudent one; indeed, the patient eventually received a diagnosis of invasive H influenzae infection, which is very rare among young, healthy individuals.
Virginia Kaldas, MD, is a third-year pediatric resident at Lincoln Medical and Mental Health Center in Bronx, New York.
Pratyusha Katta, MD, is a pediatric hospitalist at Inspira Medical Center in Vineland, New Jersey.
Irina Trifinova, MD, is a second-year pediatric resident at Lincoln Medical and Mental Health Center.
Catalina Marino, MD, is a pediatrician at Lincoln Medical and Mental Health Center.
Yekaterina Sitnitskaya, MD, is an infectious disease pediatrician at Lincoln Medical and Mental Health Center.
Shefali Khanna, MD, is chief of the Department of Pediatrics at Lincoln Medical and Mental Health Center.
References
1. Giacometti L, Chiarelli B. The skin of Egyptian mummies: a study in survival. Arch Dermatol. 1968;97(6):712-716.
2. Larzo MR, Poe SG. Adverse consequences of tattoos and body piercings. Pediatr Ann. 2006; 35(3):187-192.
3. Goldstein N. IV: complications from tattoos. J Dermatol Surg Oncol. 1979;5(11):868-878.
4. Elegino-Steffens DU, Layman C, Bacomo F, Hsue G. A case of severe septicemia following traditional Samoan tattooing. Hawaii J Med Public Health. 2013;72(1):5-9.
5. Korman TM, Grayson ML, Turnidge JD. Polymicrobial septicaemia with Pseudomonas aeruginosa and Streptococcus pyogenes following traditional tattooing. J Infect. 1997;35(2):203.
6. Dworkin MS, Park L, Borchardt SM. The changing epidemiology of invasive Haemophilus influenzae disease, especially in persons ≥65 years old. Clin Infect Dis. 2007;44(6):810-816.
7. Landgraf IM, Vieira MF. Biotypes and serotypes of Haemophilus influenzae from patients with meningitis in the city of São Paulo, Brazil. J Clin Microbiol. 1993;31(3):743-745.
8.Centers for Disease Control and Prevention. Active Bacterial Core Surveillance (ABCs) Report, Emerging Infections Program Network, Haemophilus influenzae, 2006. http://www.cdc.gov/abcs/reports-findings/survreports/hib06.pdf.
9. Resman F, Svensjö T, Ünal C, et al. Necrotizing myositis and septic shock caused by Haemophilus influenzae type f in a previously healthy man diagnosed with an IgG3 and a mannose-binding lectin deficiency. Scand J Infect Dis. 2011; 43(11-12):972-976.
10. Gorenstein A, Gross E, Houri S, Gewirts G, Katz S. The pivotal role of deep vein thrombophlebitis in the development of acute disseminated staphylococcal disease in children. Pediatrics. 2000; 106(6):E87.