
Relationship of Sexual Activity and the Heart in the Aging Male (Full title below)
Relationship of Sexual Activity and the Heart in the Aging Male: Use of the Princeton Consensus Panel Guidelines for Practical Therapy
“Diseased nature oftentimes breaks forth in strange eruption. I have more flesh than another man, and therefore more frailty” –Falstaff
Introduction
Erectile dysfunction (ED) is an early marker of penile vasculature oxidative stress and vascular dysfunction and has been suggested as a risk factor for the presence of occult cardiovascular disease (CVD).1 ED can no longer be perceived as a secondary complication of its concomitant comorbid disease states—diabetes, CVD, hypertension, and dyslipidemia. Rather, it should be recognized in a new paradigm as an early manifestation of atherosclerosis and a potentially key harbinger of vascular disease in more crucial arterial beds, such as the coronary and cerebrovascular circulation. Studies have shown that ED is an early manifestation of future cardiovascular (CV) events—atherosclerosis, vascular impairment, and vascular disease of the coronary and cerebrovascular circulation.1,2 Early intervention in men with CVD risk factors results in fewer myocardial infarctions (MIs) or other CVD outcomes than in untreated men. Therefore, it is logical that early CVD treatment intervention in men who present with ED should be beneficial, and this should be an appropriate population for primary CV prevention efforts.
However, when cardiac events do occur, it is often difficult to begin the discussion as to when it is safe to resume sexual activity. While this may not be at the forefront of the patient’s mind after the initial ‘event,’ it clearly may enter into the relationship of the couple within a few weeks of surviving the cardiac event, and the workup afterwards. With the newfound desire to engage in healthy lifestyle behaviors, the patient and his partner(s) often have questions regarding the resumption of sexual activity. This consideration and the use of erectogenic agents in the treatment of male sexual dysfunction yielded the development of what is known as the Second Princeton Consensus Panel on Sexual Dysfunction and Cardiac Risk guidelines3 for the use of oral phosphodiesterase (PDE)-inhibiting agents in the treatment of men with ED and CVD. (See section below on “Risk Stratification” for information on the original Princeton Consensus Panel guidelines.)
It is impossible to discuss the Second Princeton Consensus Panel guidelines regarding the evaluation of men with ED without examining several aspects of the relationship between sexual activity and MI, including the CV effects of sexual activity, the association between sex and MI, modulating factors that may decrease the risk of MI following sexual activity, and the treatment options for cardiac patients with sexual dysfunction.
Sexual activity is an important component of quality of life, and is therefore of great concern for both patients with heart disease and their physicians. Cardiac patients and their partners are often fearful of triggering MI during intercourse, and thus may avoid sex, especially following the vulnerable period of rehabilitation after MI. It is also well established that patients seeking medical attention for sexual dysfunction often have concomitant CVD; therefore, the determination of when it is safe to both prescribe and use erectogenic agents following MI is of great value to the practicing clinician and the cardiac patient. Urologists are at the forefront of linking their specialty to vascular disease, and it is now time for primary care clinicians and cardiologists to follow. This issue must be openly acknowledged and handled in a multidisciplinary fashion that includes both the medical and psychological impact of heart disease on sexual function, in both the affected man and his partner.
Erectile Dysfunction and Cardiovascular Disease: A “Flagging” Penis and a Broken Heart?
Schouten et al4 found that in a prospective, population-based study of 1248 Dutch men free of CVD at baseline, 258 (22.8%) had reduced erectile rigidity and 108 (8.7%) had severely reduced erectile rigidity. Investigators sought to determine the implications of this finding in relationship to impending CVD. Their methodology included the asking of a single question on the International Continence Society male sex questionnaire, “Do you get erections?”, and subsequently categorizing into: (a) no ED (self-report of “normal erections”); (b) moderate ED (self-report of erections with “reduced rigidity”); and (c) severe ED (self-report of “no erections”). During an average of 6.3 years of follow-up, in a multiple variable Cox proportional hazards model, adjusting for age and CVD risk score, the hazard ratio for a CV event was 1.6 (95% confidence interval [CI], 1.2-2.3) for the reduced erectile rigidity group and 2.6 (95% CI, 1.3-5.2) for the severely reduced erectile rigidity group. Therefore, if the man was to answer “no,” the risk of this individual developing CVD increased by 1.5 to 2.5 (similar to smoking or diabetes). In this study, the question regarding erectile rigidity proved to be a predictor for the combined outcome of acute MI, stroke, and sudden death, independent of the risk factors used in the Framingham CVD Risk Profile.
Analysis of Massachusetts Male Aging Study5 data revealed an increase in the rate of incident ED as the quartile of 10-year coronary heart disease risk increased. This implies that ED is a sensitive (although not necessarily specific) indicator of wider arterial insufficiency.5 If this could be further supported, erectile problems could call attention to coronary risk and contribute to CVD prevention efforts.
Cardiovascular Effects of Sexual Activity
Three separate components are involved in penile erection: central nervous system pathways, peripheral nervous system pathways, and the corporal bodies (corpora cavernosa and spongiosum) of the penis.6 Coital angina is angina that occurs during the minutes or hours following sexual activity.7 Coital angina appears to represent less than 5% of all anginal attacks.7 For unclear reasons, the prevalence of coital angina is higher in men than in women, and although the frequency of coitus diminishes with age in both women and men,8 sexual activity diminishes more profoundly in men following the onset of coronary artery disease (CAD).9
Coital angina is rare in patients who do not also have angina during strenuous physical exertion. It is more prevalent in sedentary individuals with severe coronary disease who experience angina with minimal physical exertion. The standard clinical measurement of physical exertion is the metabolic equivalent of the task (MET). One MET represents oxygen consumption in the resting state, equivalent to 3.5 mL/kg/minute. Sexual activity is often equated with an exercise workload of 2-3 METs in the preorgasmic phase and 3-4 METs during the orgasmic stage.10 Sexual arousal accounts for a substantial amount of the increase in oxygen consumption measured during sexual activity.10 It should be noted that few studies of oxygen consumption in older individuals have been conducted; these earlier studies were established in men with a mean age of 33 years, and thus may overstate the physical demand of sexual activity in middle-aged and older individuals.7 In general, sexual activity tends to become less vigorous in long-standing relationships in older persons over time.11
CV tolerance for sexual activity in an individual can be expressed as the functional reserve, which represents the difference between estimated peak oxygen consumption based on treadmill exercise testing and actual measurement of oxygen during sexual activity.12 Patients able to climb two flights of stairs without limiting symptoms and those who can complete stage II of a standard Bruce treadmill test (equivalent to 6-7 METs) are generally free of CV symptoms during sexual activity.13 Therefore, exercise testing is often used to assess both exercise tolerance and capacity for safely resuming sexual activity.14 The clinical implications of these observations is that sexual intercourse is associated with a modest increase in myocardial oxygen demand that lasts only for a brief time, and that sexual activity contributes only to a small percentage of MIs—in all, only 0.9% of patients with MI.15
Risk of MI After Sexual Activity
Although less than 1% of MIs occur during sexual activity, as an attributable risk, the relative risk of a nonfatal MI during and after sexual intercourse has been examined using a case-crossover method.16 The relative risk of a coital-induced MI was found to be 2.5-fold greater than during noncoital activities; the duration of exposure to this increased risk was 2 hours.16 This relative risk was threefold greater in men with a previous history of MI; however, the absolute risk of coital-induced MI is still very low, even in this high-risk group.17
The data from the Determinants of Myocardial Infarction Onset Study16 suggest that increases in myocardial oxygen demand, even if associated with ischemia, are of relatively less importance than factors likely to result in a fracture or erosion of a vulnerable atherosclerotic plaque. Once a plaque is fractured, the cascade of thrombus formation and arterial occlusion occurs.18 The mechanism for acute MI has been shown to involve coronary thrombosis secondary to the disruption of a previously nonobstructing lipid-laden plaque.18 Much of the current data on risk related to sexual activity predate the trials that have demonstrated the benefits of aspirin and statins in stabilizing plaque. Yet, these data confirm that coitus, along with exercise and episodes of significant emotional anger, are all potential triggers for MI.19 Of interest is that the higher the level of regular activity and subsequent physical endurance, the lower the likelihood that coitus will trigger an MI.18 Enhanced fitness is associated with lower heart rate and stroke volume, as well as other CV, metabolic, and autonomic effects during any given exercise level, and therefore may mediate a reduction in the potential triggering risk of sexual activity and MI.18
Other risk modifiers include medications that reduce heart rate or blood pressure or inhibit platelet aggregation. Beta blockers, which reduce myocardial oxygen demand, can minimize or eliminate angina during sexual intercourse. The Determinants of Myocardial Infarction Onset Study,16 however, found that beta blockers reduced the risk of MI following anger19 but not sexual intercourse.15 Aspirin lowers the risk of MI following episodes of anger19 and in the morning waking hours,20 both of which are known triggers of MI. However, in the Determinants of Myocardial Infarction Onset Study, aspirin therapy was associated with a nonsignificant reduction in the relative risk of MI following sexual activity.19
Risk Stratification of Individuals Who Resume Sexual Activity Following MI According to the Second Princeton Consensus Panel Guidelines
A singular issue of this review is when sexual activity can be safely resumed following an acute MI. This was addressed by the original Princeton Consensus Panel in 2000 with the development of a classification system for stratification of patients into high-, low-, and intermediate-risk categories of cardiac risk.17 The recommendations of this multispecialty panel found that the majority of patients are in the low-risk category, which includes patients with (1) controlled hypertension; (2) mild, stable angina; (3) successful coronary revascularization; (4) a history of uncomplicated MI (remote); (5) mild valvular disease; and (6) no symptoms and fewer than three CV risk factors. It was felt that these patients could safely resume or initiate sexual activity or receive treatment with oral erectogenic agents. Of course, the important exception is the use of sildenafil—which was the only available phosphodiesterase type 5 (PDE-5) agent in 2000—in those patients taking nitrates in any form.
In this stratification, patients in the intermediate-risk category include those with (1) moderate angina; (2) a recent MI (within 6 wk); (3) left ventricular dysfunction and/or class II congestive heart failure (ejection fraction < 40%); (4) nonsustained low-risk arrhythmias; and (5) more than three risk factors for CAD. It was felt that these patients should receive further cardiologic evaluation before restratification into the low- or high-risk category.
Patients in the high-risk category include those with (1) unstable or refractory angina; (2) uncontrolled hypertension; (3) class III or IV congestive heart failure; (4) very recent MI (within 2 wk); (5) high-risk arrhythmias; (6) obstructive cardiomyopathies; and (7) moderate-to-severe valvular disease. These patients should be stabilized by specific treatment for their cardiac condition before resuming sexual activity or being treated for sexual dysfunction.17
This stratification of patients into graded cardiac risk may assist in the clinical management and facilitating discussion of the incidence of cardiac events and sexual activity following MI. The panel addressed when to safely resume erectogenic drugs by concluding that men in the low-risk category could safely use sildenafil as long as there was no concomitant use of nitrates. Without addressing the direct timing of the use of these drugs, the American College of Cardiology (ACC)/American Heart Association (AHA) guidelines suggest that sexual activity with a usual partner in patients considered low risk following uncomplicated MI could be resumed after 10 days.21 Other sources suggest waiting 2 weeks.18
The recent emergence of epidemiologic studies underscoring the association between CV risk factors and sexual dysfunction,5,22-26 pharmacologic interactions of the three presently available PDE-5 inhibitors (sildenafil, tadalafil, and vardenafil), and their potential CV benefits27-30 underscored the need for the Second Princeton Consensus Conference. This meeting was held in June 2004, and the guidelines have since been published.3
The new consensus report upholds the Princeton I algorithm for treating ED in patients with CVD, in which the patient is assigned to one of three risk categories. However, the new guidelines discuss special management strategies for treating patients who have CVD with PDE-5 inhibitors, particularly those in emergency medical situations. Furthermore, the report recommends that all patients should be reassessed at regular intervals (eg, every 6 mo).3
Exercise tolerance, ascertained by medical history, can guide the clinician in determining the CV risk of sexual activity. The panel recommends that the ability to perform exercise of modest intensity (≥ 6 METs) without symptoms generally indicates a low risk of CVD. With respect to management strategies, the benefits of lifestyle modification (such as weight loss and increased physical activity) were explored, especially for patients with ED who are at high risk for CVD.3
In most patients with angina, functional reserve is greater than that required by sexual activity.7 However, because mild or well-controlled angina does not exclude serious CAD, it is also recommended that these patients undergo noninvasive evaluation. The relative risk of a coitus-induced coronary event is no greater in patients with established coronary disease than in those without documented cardiac disease, as suggested above. The antianginal drug regimen may need to be modified to accommodate drug therapy for ED; for example, eliminating the need for oral or topical nitrates and implementation of more selective beta and apha blocker combination agents, currently in use in clinical practice.
The risk of sexual activity following coronary artery bypass grafting or percutaneous coronary intervention is inversely related to the adequacy of revascularization. Exercise stress testing may be of benefit in assessing the extent and severity of residual ischemia. Patients without significant residual ischemia should be considered low risk.3
Patients with a past MI who are currently asymptomatic, do not exhibit treadmill-induced ischemia, or have undergone coronary revascularization are at low risk for coital MI. Traditionally, it has been recommended that patients avoid sex for 6-8 weeks following an MI; however, this may be reduced to 3 or 4 weeks in patients without treadmill-induced ischemia and in those who have undergone coronary revascularization. Exercise training after acute MI improves CV efficiency and reduces myocardial oxygen consumption during customary activities, including sexual activity. Cardiac rehabilitation exercise programs are helpful in reducing coital symptoms and coital heart rates.3
A patient with a recent MI (within 2 wk) still remains at high risk. This patient may be at risk for coital-induced reinfarction, cardiac rupture, or coital-induced arrhythmias. Because the period of maximum risk appears to be the first 2 weeks after MI, sexual activity is generally not recommended during this period. At present, there are insufficient data to evaluate the risk of patients with acute MI who have undergone complete revascularization in the acute phase.3
The final algorithm for risk stratification and patient management views the assessment of patients with ED as a three-step process:
1. Assessment of sexual dysfunction should be incorporated into the initial CV evaluation for all men. Further clinical evaluation based on a history, physical examination, and relevant laboratory results enables stratification of patients into high, low, or intermediate levels of cardiac risk. Specialized CV testing is recommended to reclassify patients at intermediate risk into the low- or high-risk category (Figure).

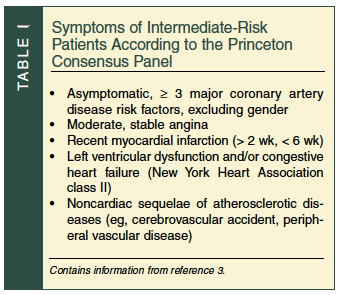 2. Most patients at low risk may safely engage in sexual activity or receive treatment for ED as needed. Patients at high risk should be stabilized by cardiologic treatment before resumption of sexual activity is considered or treatment of sexual dysfunction is recommended. Patient follow-up and reassessment at regular intervals is recommended (Table I).
2. Most patients at low risk may safely engage in sexual activity or receive treatment for ED as needed. Patients at high risk should be stabilized by cardiologic treatment before resumption of sexual activity is considered or treatment of sexual dysfunction is recommended. Patient follow-up and reassessment at regular intervals is recommended (Table I).
3. Atherosclerotic disease involving the coronary, brain, or peripheral circulation shares common risk factors with ED. Moreover, ED may be an early or sole symptom of CVD. Accordingly, an evaluation of CV risk factors should be performed routinely in patients presenting with ED. Measures for improving and monitoring the risk profile and evaluation for subclinical CVD should be included in the discussion with all patients. This is vital, and should be considered a first and priority step before the initiation of ED therapy.3
Resumption of PDE-5 Therapy Following MI
Sexual dysfunction is common in patients with CVD and after MI because of concern about risk, side effects of medications, the coexistence of shared risk factors (dyslipidemia, diabetes, smoking, and hypertension), and the presence of psychological factors.5,26,31-38 It is estimated to occur in 50-75% of patients following MI.25,26,31-38
Cardiac patients may have psychological causes for sexual dysfunction related to the suddenness of the event that include worries about triggering an MI or sudden death, depression following MI, and anxiety about a newly diagnosed illness.34,35,39-41 However, many physicians do not discuss the issue of sexual intercourse with patients following MI. For these men and women, attendance at cardiac rehabilitation, treatment of any psychiatric condition, and reassurance of the low attributable risk of MI may improve sexual function. Because sexual activity is equated with physical activity, exercise testing is often used to measure exercise tolerance and, therefore, tolerance for the risk of sexual activity.
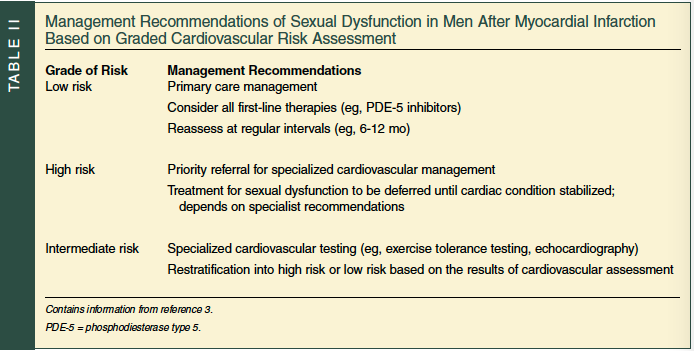
In general, the management of sexual dysfunction in patients after MI is based upon the estimated risk as delineated in the Second Princeton Consensus Panel (Table II). This stepwise risk stratification relies on coronary risk factors, historical features, and the results of specialized cardiac testing.3 It is designed to distinguish the great majority of patients (60-70%) who are at low risk from the minority of patients (10-15%) who are at high risk.42 Intermediate-risk patients (15-30%) require specialized cardiac testing for reclassification into the low- or high-risk category. Exercise testing enables an objective assessment of exercise tolerance and also helps to identify prognostic markers, such as heart rate, blood pressure, and workload, at which symptoms of angina, dyspnea, and fatigue appear.43 Low-risk male patients with ED can be treated with a PDE-5 inhibitor without undergoing further diagnostic testing. High-risk patients should undergo cardiac assessment and be appropriately treated before being considered for PDE-5 inhibitors. Treatments may include combination pharmacotherapy, such as beta blockers, angiotensin-converting enzyme inhibitors, statins, and antiplatelet agents; percutaneous coronary interventions; and coronary artery bypass graft surgery.17
The three PDE-5 inhibitors available in the United States (sildenafil, vardenafil, and tadalafil) have been demonstrated to be safe for most men with ED.44,45 However, deaths from CAD have occurred following sexual activity in a few men who have taken these drugs.46 Nitrate administration, presumably for coital angina, was implicated in approximately 20% of the deaths that occurred in patients who had received sildenafil.46 Hypotension resulting from this interaction may transform coital angina from a potentially reversible situation into an irreversible one. Although the actual frequency of marked hypotension resulting from the PDE-5 inhibitor–nitroglycerin combination is largely unknown for patients experiencing coital angina, the ACC/AHA recommendation to avoid nitrates for at least 24 hours after taking short-acting PDE-5 inhibitors is well advised,13,15,21 and 48 hours after taking tadalafil.43
Let us return briefly to the relationship of ED and CAD. Indeed, Gazzaruso et al47 recruited 291 men with type 2 diabetes and silent CAD and found that those patients who developed major adverse cardiac events (MI and cardiovascular accident) over the course of 4 years were more likely to have ED (61%) than those without ED (36%). Of note in this study, statin use significantly reduced major cardiac events, and there was a trend (although not statistically significant) for PDE-5 use to also be associated with a lower rate of cardiac events. In addition, it has been postulated that daily PDE-5 inhibitor therapy may be synergistic with angiotensin II receptor blockers (ARBs) to not only lower blood pressure but also to reverse ED.48 With regard to future use of PDE-5 inhibitor therapy, such therapy taken daily may improve not only erectile function, but heart health in general and particularly endothelial function.49 It is indeed possible that in aging men we will find a use for these and other medications to reduce overall CV risk and treat sexual dysfunction simultaneously.
Conclusions
Only approximately 5% of anginal attacks and less than 1% of MIs are brought on by sexual activity. In most cases, coital angina can be managed like any other angina. PDE-5 inhibitors can be safely used by many patients who have both CVD and ED. However, the concomitant use of nitrates and these drugs may lead to a profound hypotension and is strictly contraindicated. Following MI, patients should be categorized into low-, intermediate-, or high-risk groups following the Second Princeton Consensus Panel guidelines. Focus should be directed to effort or exercise tolerance after MI, often clarified by exercise cardiac testing. Those patients who fall into the low-risk category may be safely treated with PDE-5 inhibitors after at least 4 weeks following MI. Physicians should counsel patients regarding sexual activity after MI and, in particular, address the psychological factors, physiological factors, and exercise tolerance, as well as the treatment of any coital angina following PDE-5 use with the patient and partner. With regard to future use of PDE-5 inhibitor therapy, such therapy taken daily may improve not only erectile function, but heart health in general and particularly endothelial function. This concept of dual therapy, PDE-5 medications and statins or ARBs, may not only improve adherence with therapy, but also serve to drive down costs by expanding the role of such therapy. Dr. Miner reports that he is a consultant for Sanofi Aventis and GSK, and has received research grants from GSK and Indevus.
Dr. Nehra reports that he is a consultant for Sanofi, GSK, and Pfizer.
Dr. Tilkemeier reports no relevant financial relationships.
Dr. Miner is Co-Director, Men’s Health Center at The Miriam Hospital, and Clinical Associate Professor of Family Medicine, The Warren Alpert Medical School, Brown University, Providence, RI; Dr. Tilkemeier is Director of Cardiac Rehabilitation at The Miriam Hospital, and Associate Professor of Medicine, The Warren Alpert Medical School, Brown University; and Dr. Nehra is Professor of Urology, Department of Urology, Mayo Clinic College of Medicine, and Consultant, Mayo Clinic, Rochester, MN.