
Septic Hip, or Transient Synovitis? Assessing the Diagnostic Utility of Ketorolac Administration in Children
ABSTRACT: To evaluate the use of ketorolac to help distinguish between septic arthritis of the hip and transient synovitis of the hip in pediatric patients, a retrospective review was performed of the charts of 211 patients at a level I children’s hospital with possible septic hip or transient synovitis over a 3-year period. The patients’ Kocher diagnostic criteria results, operating room (OR) findings, and whether or not ketorolac was administered were recorded. Hospital admissions, OR admissions, and total emergency department (ED) times of children who received ketorolac were compared with those of children who did not receive ketorolac. Administering ketorolac was not found to affect the number of patients admitted to the hospital or the OR, or to affect total ED time. Anecdotal evidence suggested, however, that ketorolac may be of diagnostic benefit in differentiating a septic hip from transient synovitis.
Septic arthritis of the pediatric hip has severe sequelae and limited treatment options if it is undiagnosed or misdiagnosed. It is, therefore, a surgical emergency when diagnosed. Expeditious diagnosis followed by drainage of the hip is essential for good outcomes. Traditionally, once septic arthritis of the hip is diagnosed, the patient is taken immediately to the operating room (OR) for open surgical aspiration and drainage.1-3 Other treatment options, such as arthroscopic lavage and serial ultrasound-guided drainage, also have been used.4,5
The difficulty in the management of septic hip in the pediatric population lies perhaps foremost in its diagnosis. Patients with transient synovitis of the hip, which is managed medically, often present to the pediatrician’s office or emergency department (ED) with similar symptoms. Both patients also may have similar clinical examination results and laboratory values. Therefore, the goal is to differentiate between these two populations and expeditiously manage patients with septic hips without unnecessarily exposing patients with transient synovitis to surgical intervention.
Most providers follow the criteria developed by Kocher and colleagues, which evaluate whether a patient has a core temperature of greater than 38.5°C, has a white blood cell (WBC) count greater than 12,000/µL, has an erythrocyte sedimentation rate (ESR) greater than 40 mm/h, and is unable to bear weight.6,7 The greater the number of positive findings, the higher likelihood the patient has a septic hip rather than transient synovitis. If 3 or 4 criteria are positive, then the likelihood of a septic hip is greater than 90%. Other authors developing criteria for differentiating between these two entities have identified similar factors.8,9
Some patients, however, present diagnostic difficulties despite the application of these criteria. It is common to encounter patients with 2 or even 3 positive criteria who, after a thorough physical examination, still do not give the appearance of having a septic hip. Other investigators have described such a dilemma, where the predicted probability of a septic hip using the original Kocher criteria does not match their patient populations as well as in the original study.10,11 One of these studies10 evaluated patients using the 4 Kocher criteria, and the other used 5 criteria—the 4 Kocher criteria, plus C-reactive protein (CRP) level11; in both studies, the predicted probability of septic arthritis was approximately 60% if all criteria were positive. Another study found that WBC count and ESR had poor sensitivity and specificity for a septic hip.12 Yet another study evaluated weight-bearing status, temperature, WBC count, and CRP and found that only weight-bearing status and CRP were the critical variables.13
No previous study has evaluated the use of medical treatment to help distinguish between a septic hip and transient synovitis of the hip in pediatric patients. Traditionally, transient synovitis of the hip due to a viral inflammation is managed with nonsteroidal anti-inflammatory drugs (NSAIDs), most commonly ibuprofen.14 Ideally, the medical management would be powerful enough to rapidly improve the symptoms of transient synovitis of the hip without masking symptoms of a septic hip. In our practice, if a patient seems to have a particularly difficult diagnosis, we recommend a dose of ketorolac in the hopes of seeing a rapid resolution of symptoms if they are related to viral inflammation.
The purpose of this study was to determine whether ketorolac can be used to help distinguish between transient synovitis of the hip and septic hip, particularly in pediatric patients with a difficult diagnosis. The hypothesis was that administration of ketorolac would decrease the number of patients admitted to the hospital, the number of patients admitted to the OR, and the total ED time for patients with transient synovitis of the hip.
Materials and Methods
Institutional review board approval was obtained prior to initiating the study. A search of the ED database at a level I children’s hospital was then carried out to identify all patients with the possibility of a septic hip or transient synovitis who had been seen over a 3-year period. The diagnoses and terms used for the search were septic arthritis, toxic synovitis, hip pain, leg pain, thigh pain, knee pain, lower extremity pain, hip effusion, fever, febrile illness, viral syndrome, myositis, muscle strain, ataxic gait, and limp.
The initial search produced 348 records. All of these records then underwent a chart review. The 137 records in which the patient’s history, examination findings, and diagnosis ruled out both septic hip and transient synovitis were excluded from further review. A total of 211 remaining records either carried a diagnosis of septic hip or transient synovitis, or had a diagnosis that was unclear and concerning for either condition, such as the patient depicted in Figure 1. 
All of these 211 charts then were reviewed in more detail, and a number of variables were documented for each, including the patient’s age; the duration of symptoms; the results of assessment using the 4 Kocher criteria; whether or not the patient received ketorolac or other NSAIDs; the total ED time (ie, the time from the first physician evaluation that was documented in the chart to the patient’s discharge from the ED); whether or not the patient was admitted to the hospital; whether or not the patient was admitted to the OR; and OR findings.
The charts also were evaluated a minimum of 1 year forward from the time of the ED visit to identify any instances of patients returning later with a diagnosis of septic hip or transient synovitis and to identify any instances of adverse events related to ketorolac administration.
Treatment Algorithm
At our institution, a patient with signs and symptoms that raise significant clinical concern for a septic hip is taken to the OR for aspiration with irrigation and debridement. Arranging conscious sedation for pediatric patients in the radiology suite can be difficult and often requires waiting until the following day. Consequently, we generally do not have the liberty of waiting for ultrasonography-guided aspirations for patients whose presentation is concerning for a septic hip, and they are transferred to the OR. Ultrasonography is used infrequently for this patient population.
However, it is common for these patients to receive ketorolac as they are being sent to the preoperative holding area. A patient who receives ketorolac is reexamined in the holding unit; if the examination results show significant improvement after ketorolac is given, the patient may be admitted for observation without urgent aspiration at the discretion of the attending physician. Patients who do not require urgent admission to the OR based on clinical suspicion (such as those with 2 or fewer positive Kocher criteria), but who remain concerning for a septic hip, also may receive ketorolac.
Statistical Analysis
Of all patients with at least 3 positive Kocher criteria, those who received ketorolac were compared with those who did not in terms of hospital admission and OR admission; this was done using the Pearson χ2 test. The hospital and OR admissions of patients who received ketorolac, those who received other NSAIDs only, and those who received no medications also were compared, again using the Pearson χ2 test.
Of all patients with at least 3 positive Kocher criteria, those who received ketorolac were compared with those who did not in terms of total ED time; this was done using a 2-sample t test with unequal variances. The total ED time of patients who received ketorolac, those who received other NSAIDs only, and those who received no medications also were compared using 1-way analysis of variance.
All of these statistical analyses then were performed for patients with at least 2 positive Kocher criteria.
Results
During the study period, 2 patients were found to have had a septic hip, one with positive cultures for Streptococcus pyogenes, the other for Kingella kingae. Two additional patients underwent hip aspiration and drainage but had negative culture results. Three patients were prepared for the OR because of an ED workup concerning for septic hip. However, shortly before discharge from the ED, the 3 patients were given ketorolac. Upon examination in the preoperative area, these 3 patients demonstrated significant improvement and therefore no longer required surgical intervention. They were admitted for observation and were monitored for 1 to 2 days until there was no longer clinical concern for septic hip (Figure 2). All 7 of these patients had good outcomes, and none had recurrence of symptoms concerning for a septic hip. In addition, no patients with a diagnosis other than septic hip, including transient synovitis, presented later with symptoms concerning for a septic hip. No adverse events related to the administration of ketorolac were reported. 
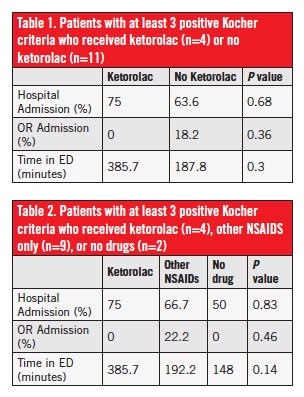
For all patients with at least 3 positive Kocher criteria, there were no statistically significant differences in hospital admission, OR admission, or total ED time between patients who received ketorolac and patients who did not receive ketorolac (Table 1). There also were no statistically significant differences in these values when comparing patients who received ketorolac, patients who received other NSAIDs only, and patients who received nothing (Table 2). For all patients with at least 2 positive Kocher criteria, there were no statistically significant differences in OR admission or total ED time between patients who received ketorolac to patients who did not receive ketorolac (Table 3). There also were no statistically significant differences in these values when comparing patients who received ketorolac, patients who received other NSAIDs only, and patients who received nothing (Table 4).
The only statistically significant finding was that among patients with at least 2 positive Kocher criteria, more patients who received ketorolac were admitted to the hospital than those who did not receive ketorolac.
Discussion
For patients with at least 3 positive Kocher criteria, ketorolac treatment did not affect the number of hospital or OR admissions, and it did not affect the total ED time. Patients with at least 2 positive Kocher criteria who received ketorolac were more likely to be admitted. Ketorolac treatment did not affect the number of OR admissions or the total ED time in patients with at least 2 positive Kocher criteria. A total of 2 of the 211 study subjects were diagnosed with a septic hip.
The small number of patients in the study with a septic hip diagnosis makes it impossible to confirm the safety of ketorolac in the setting of a septic hip. Nevertheless, we did not identify any patients whose treatment was delayed by the masking of septic hip symptoms after ketorolac administration.
This study was conducted at a level I children’s hospital that serves as a tertiary referral center for a population of between 1 million and 1.5 million residents. The hospital has agreements with all of the hospitals in the catchment area such that any pediatric patient with a workup at all concerning for septic hip will be transferred to its referral center ED. Because of this arrangement, all of the patients managed at our center for septic hip or transient synovitis would return to our facility for recurring symptoms concerning for septic hip. While it is impossible to be 100% certain, this arrangement allows us to feel confident that no patients who received ketorolac had symptoms of a septic hip masked by the drug and were at risk of having a delay in treatment. In other words, the most likely scenario is that all patients with septic hip during the study period were identified and no patients received treatment elsewhere, resulting in a treatment delay, because of the administration of ketorolac.
The small number of patients with confirmed septic hip also likely impacted the ability to detect differences in the variables studied. Anecdotally, however, it has been our experience that ketorolac administration does indeed help in the diagnosis of difficult cases of transient synovitis. Despite the proven utility of the Kocher criteria, studies have shown that the criteria may have variable predictability depending on setting; therefore, the diagnosis of a septic hip remains a clinical one.10-13 Indeed, in our study, only 7% (1 of 15) of patients with 3 or more positive Kocher criteria were diagnosed with a septic hip, and the additional study subject with a septic hip had only 2 positive criteria.

Ketorolac treatment may enhance clinical decision-making in this setting and serve as a valuable diagnostic tool to facilitate standardization of care between the orthopedic, pediatric, and emergency department staffs. This approach could help prevent unnecessary hospital admissions or trips to the OR, such as was seen in the 3 patients who went to the OR preoperative holding area, only to improve after receiving ketorolac. These 3 patients, who initially presented with very concerning examination findings that otherwise would have led to aspiration, were spared the procedure as a result of a rapid response to ketorolac administration.
The one statistically significant finding in this study—that patients receiving ketorolac were more likely to be admitted to the hospital—is somewhat surprising at first glance. This finding is likely explained by the fact that the patients who received ketorolac were the same subjects with workup results that were more concerning for a septic hip. In such a patient, the orthopedic service generally is consulted, and it often is the orthopedic surgeon, rather than the ED physicians, who recommends a dose of ketorolac. The patients most likely to be admitted to the hospital because of a concerning workup also are the patients most likely to be seen by the orthopedic service and, subsequently, the most likely to receive ketorolac. The same idea likely explains the observations about total ED time, although the results were not statistically significant; the likely reason that patients receiving ketorolac had longer ED times is that they also were the patients with more concerning findings for septic hip.
Study Limitations
The results of this study must be seen in light of the study’s limitations. First, it was difficult to control for all confounding variables. Because of the retrospective nature of this study, we were unable to ensure that all patients received identical workups. This means that not all patients with similar histories and examination findings received similar medications or had the same laboratory workup.
Given that study subjects were identified strictly through ED records, some patients with a septic hip who were treated at our institution could have been admitted directly through the office of their pediatrician. Although this is a rare occurrence, it would mean that those patients were not included in this study, and this fact could help explain the small number of septic hip cases in our search.
Finally, despite the relatively large number of subjects, the study likely is underpowered to detect a difference in the variables studied owing to the small number of patients with a septic hip.
In light of the observations from this study, we believe that it would be beneficial for a prospective study to be conducted that evaluates whether using ketorolac in pediatric patients with a equivocal diagnosis between septic hip and transient synovitis would reduce the number of hospital and OR admissions and perhaps even speed ED management times. If ketorolac could help distinguish septic hip and transient synovitis, it would be not only therapeutic but also diagnostic. The safety of ketorolac in the management of pediatric septic hip also needs to be further evaluated in terms of medication adverse events and masking of symptoms.
The clinical significance of this retrospective study is that while ketorolac did not decrease hospital admissions or OR admissions, or expedite ED times, anecdotal evidence suggests that ketorolac may be beneficial in the setting of diagnostic dilemmas between septic hip versus transient synovitis in pediatric patients.
Obviously, caution must be used when administering ketorolac to any patient with findings concerning for a septic hip. Care should proceed as usual for potential septic hip patients until it becomes clear that the patient no longer has significant findings that are concerning for septic hip. In such cases, the patient still should be followed up closely to monitor for the return of any signs of septic hip.
Conclusion
Administering ketorolac to pediatric patients with a workup that is concerning for septic arthritis of the hip or for transient synovitis of the hip did not affect the number of patients admitted to the hospital, the number of patients admitted to the operating room, or the total emergency department time. Administering the medication may, however, be helpful in distinguishing transient synovitis of the hip from septic hip in pediatric cases with workup results that are more concerning for septic hip.
Marc Tompkins, MD, is an orthopedic surgeon and assistant professor in the Department of Orthopaedic Surgery at the University of Minnesota Medical School in Minneapolis.
Benjamin G. Bruce, MD, is an orthopedic surgeon at the Sports and Orthopedic Center in Boca Raton, Florida.
Craig P. Eberson, MD, is an associate professor and director of the Orthopedic Residency and the Pediatric Orthopedic Surgery Fellowship at the Warren Alpert Medical School of Brown University. He also is chief of the Division of Pediatric Orthopedic Surgery and Scoliosis at Hasbro Children’s Hospital, the pediatric division of Rhode Island Hospital, in Providence.
Acknowledgement
The authors thank Steven E. Reinert, MS, at the Lifespan health system in Providence, Rhode Island, for his assistance with the statistical analysis.
References
1. Herndon WA, Knauer S, Sullivan JA, Gross RH. Management of septic arthritis in children. J Pediatr Orthop. 1986;6(5):576-578.
2. Kocher MS, Mandiga R, Murphy JM, et al. A clinical practice guideline for treatment of septic arthritis in children: efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am. 2003;85(6):994-999.
3. Smith MJ, White RA, Gainor BJ. Combined technique for draining septic arthritis of the pediatric hip. Am J Orthop (Belle Mead NJ). 2007;36(3):165-166.
4. El-Sayed AMM. Treatment of early septic arthritis of the hip in children: comparison of results of open arthrotomy versus arthroscopic drainage. J Child Orthop. 2008;2(3):229-237.
5. Givon U, Liberman B, Schindler A, Blankstein A, Ganel A. Treatment of septic arthritis of the hip joint by repeated ultrasound-guided aspirations. J Pediatr Orthop. 2004;24(3):266-270.
6. Kocher MS, Mandiga R, Zurakowski D, Barnewolt C, Kasser JR. Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am. 2004;86(8):1629-1635.
7. Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm. J Bone Joint Surg Am. 1999;81(12):1662-1670.
8. Caird MS, Flynn JM, Leung YL, Millman JE, D’Italia JG, Dormans JP. Factors distinguishing septic arthritis from transient synovitis of the hip in children: a prospective study. J Bone Joint Surg Am. 2006;88(6):1251-1257.
9. Jung ST, Rowe SM, Moon ES, Song EK, Yoon TR, Seo HY. Significance of laboratory and radiologic findings for differentiating between septic arthritis and transient synovitis of the hip. J Pediatr Orthop. 2003;23(3):368-372.
10. Luhmann SJ, Jones A, Schootman M, Gordon JE, Schoenecker PL, Luhmann JD. Differentiation between septic arthritis and transient synovitis of the hip in children with clinical prediction algorithms. J Bone Joint Surg Am. 2004;86(5):956-962.
11. Sultan J, Hughes PJ. Septic arthritis or transient synovitis of the hip in children: the value of clinical prediction algorithms. J Bone Joint Surg Br. 2010;92(9):1289-1293.
12. Li SF, Cassidy C, Chang C, Gharib S, Torres J. Diagnostic utility of laboratory tests in septic arthritis. Emerg Med J. 2007;24(2):75-77.
13. Singhal R, Perry DC, Khan FN, et al. The use of CRP within a clinical prediction algorithm for the differentiation of septic arthritis and transient synovitis in children. J Bone Joint Surg Br. 2011;93(11):1556-1561.
14. Kermond S, Fink M, Graham K, Carlin JB, Barnett P. A randomized clinical trial: should the child with transient synovitis of the hip be treated with nonsteroidal anti-inflammatory drugs? Ann Emerg Med. 2002;40(3):294-299.