
Slipping Rib Syndrome
A 16-year-old girl presented with a history of chronic epigastric and right upper quadrant abdominal pain for years. The pain was sharp and was not associated with nausea, vomiting, or a change in bowel habits.
In the past, the patient had undergone an extensive gastrointestinal (GI) workup, including screening blood tests, abdominal computed tomography (CT), and abdominal ultrasonography, the results of which were normal. Upper GI endoscopy had shown chronic gastritis, which had been treated with a proton-pump inhibitor; still, her pain persisted. Results of a hepatobiliary iminodiacetic acid scan had shown a low gallbladder ejection fraction, for which she had undergone laparoscopic cholecystectomy and appendectomy. The postprocedural pathology report suggested chronic cholecystitis and a normal appendix.
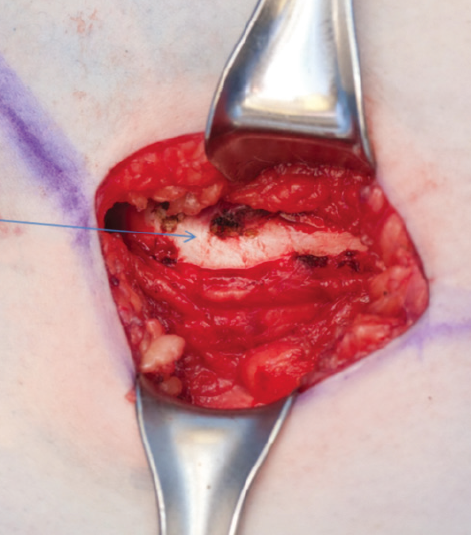
Intraoperative photograph showing the 10th rib; the 11th rib has slipped underneath the 10th rib, placing pressure on the intercostal nerve and leading to the patient's multiyear history of chronic right upper quadrant abdominal pain.
The patient continued to have significant abdominal pain. She recently experienced right-sided chest pain. A chest CT scan and electrocardiography were done, the results of which were normal. Counseling therapy and a trial of amitriptyline, 75 mg daily, had failed to relieve her pain. This chronic pain was causing significant distress and had forced her to drop out of school. The pain also had led to significant weight gain (body mass index, 32.2 kg/m2) due to poor physical activity.
On physical examination at our clinic, her pain was confined to the right lower rib area. The pain was reproducible by palpation, with a palpable click upon pushing on the right lower rib. A gastric accommodation test was performed, the results of which were normal. A review of her chest CT scans confirmed normal results. Consultation with pediatric surgery was requested; the results of the physical examination performed by the pediatric surgeon were consistent with our results. A diagnosis of slipping rib syndrome was suspected. A trial of local anesthetic injections (intercostal nerve block) failed to relieve the patient’s pain, and she was scheduled for surgery.
The patient underwent an abdominal incision directly above the right 10th rib. Exposing the right lower rib area revealed that the 11th rib had slipped underneath the 10th rib and was pressing on the intercostal nerve. This most likely was the cause of her pain, so her 10th and 11th costal cartilages and 11th rib were excised by blunt dissection and electrocautery.
At a 4-week postsurgical follow-up visit, the patient reported complete resolution of her epigastric and right upper quadrant pain.
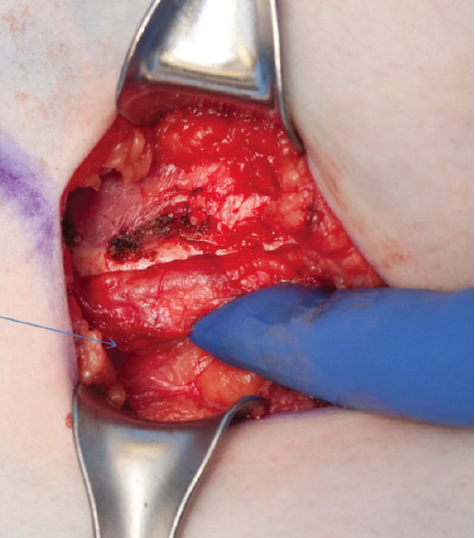
Intraoperative photograph showing the 11th rib after it was brought out from under the 10th rib. The 10th and 11th costal cartilages and 11th rib subsequently were excised, leading to complete resolution of the patient’s pain.
Slipping rib syndrome, a rare cause of abdominal pain, often is misdiagnosed or undiagnosed, which can lead to months or years of unresolved abdominal and/or thoracic pain, as was the case with our patient. Children with slipping rib syndrome often undergo extensive diagnostic evaluation and experience a prolonged course of abdominal or chest pain and accompanying psychological problems before receiving the proper diagnosis.
Slipping rib syndrome’s etiology is not well understood, but surgical findings suggest that the condition arises from hypermobility of the costal cartilage of the false ribs (ribs 8, 9, and 10),1 which often leads to the affected rib slipping under the superior adjacent rib.2 This can cause irritation of the intercostal nerve,3 strain of the intercostal muscles,4 sprain of the lower costal cartilage,5 or general inflammation in the affected area.
The diagnosis is suspected in the presence of direct tenderness over the involved cartilages or a positive response to the hooking maneuver. The hooking maneuver consists of placing the fingers under the lowest costal cartilage on the involved side and drawing them anteriorly, reproducing the patient’s pain and eliciting a clicking sensation. The contralateral side serves as a control. The diagnosis is supported by temporary relief of symptoms with intercostal block.6
While reassurance and avoidance of troubling movements is adequate therapy for most adult patients,4 this approach likely is impractical for children. Intercostal block with local injection of anesthetics and corticosteroids may relieve pain temporarily. Subperichondrial resection of the involved costal cartilages, with careful protection of the intercostal nerves, is effective in relieving the pain in children.7
References:
1.
Gregory PL, Biswas AC, Batt ME. Musculoskeletal problems of the chest wall in athletes. Sports Med. 2002;32(4):235-250.
2.
Copeland GP, Machin DG, Shennan JM. Surgical treatment of the ‘slipping rib syndrome.’ Br J Surg. 1984;71(7):522-523.
3.
Mooney DP, Shorter NA. Slipping rib syndrome in childhood. J Pediatr Surg. 1997;32(7):1081-1082.
4.
Arroyo JF, Vine R, Reynaud C, Michel JP. Slipping rib syndrome: don’t be fooled. Geriatrics. 1995;50(3):46-49.
5.
Blackman NS. Slipping rib syndrome with review of related anterior chest wall syndromes. N Y State J Med. 1963;63:1670-1675.
6.
Abbou S, Herman J. Slipping rib syndrome. Postgrad Med. 1989;86(6):75-78.
7.
Fu R, Igbal CW, Jaroszewski DE, St. Peter SD. Costal cartilage excision for the treatment of pediatric slipping rib syndrome. J Pediatr Surg. 2012;47(10):1825-1827.