
Supporting Caregivers in Ethnically Diverse Communities: Focus on Alzheimer’s Disease
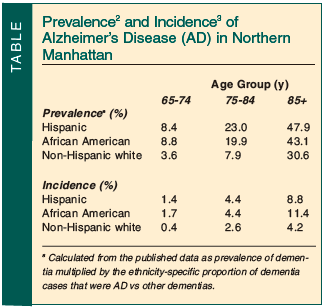
According to the Alzheimer’s Association, approximately 5.1 million people, or one out of eight people over the age of 65, currently have Alzheimer’s disease (AD). By the year 2030, the number of Americans with this progressive neurologic disorder will reach nearly 7.7 million, and by 2050, between 11 and 16 million.1 The risk of AD is significantly elevated in the African-American and Hispanic populations. Prevalence rates of all types of dementia, including AD, are higher in these groups as compared with non-Hispanic white individuals.2 African-American and Hispanic-American persons have approximately two times the incidence rates for AD as their non-Hispanic white counterparts, at 4.2% per person-year for African Americans, 3.8% per person-year for Hispanic Americans, and 1.9% for non-Hispanic white individuals3 (see Table for age-specific incidence rates). The Multi-Institutional Research in Alzheimer’s Genetic Epidemiology (MIRAGE) study4 found a cumulative relative risk (RR) of 1.6 (95% confidence interval [CI], 1.4-1.9) in African-American first-degree blood relatives of patients with AD, as compared with white individuals.
 When first recognized, AD appears to be more advanced in African-American populations.2,5 Several explanations have been offered to account for the discrepancy in rates of early detection of AD found between the groups. In one study, a national sample of 1176 adults age 35 and older (48.6% white, 25.7% African American, and 25.8% Hispanic-American) showed that African-American and Hispanic- American respondents were significantly more likely to believe that AD is a normal part of aging.6
When first recognized, AD appears to be more advanced in African-American populations.2,5 Several explanations have been offered to account for the discrepancy in rates of early detection of AD found between the groups. In one study, a national sample of 1176 adults age 35 and older (48.6% white, 25.7% African American, and 25.8% Hispanic-American) showed that African-American and Hispanic- American respondents were significantly more likely to believe that AD is a normal part of aging.6
While no cure exists for the disease, early diagnosis and treatment is the optimal way to manage the symptoms of AD. Existing agents for the treatment of AD now cover all stages of AD and offer hope that dementia can be slowed. Treatment options include the cholinesterase inhibitors (ChEIs) rivastigmine and galantamine, both approved for treatment of mild-to-moderate AD, and donepezil, which is approved for treatment of mild, moderate, and severe AD. For patients with moderate-to-severe AD, memantine can be added to a ChEI such as donepezil. It is neither necessary nor desirable to discontinue the ChEI when memantine is initiated.
To enhance early detection, screening for dementia should become a part of the routine physical examination for all patients age 65 and older. The Mini-Cog exam can help to increase the number of possible AD cases identified in the primary care setting without making undue demands on physician time.7 It comprises a three-item recall task and a clock-drawing exercise. In validation studies, it has proven superior to the Mini-Mental State Examination (MMSE) in predicting dementia, even in a poorly educated, non-English–speaking population. Administering the Mini-Cog exam takes approximately 3 minutes—less than half the time required for the MMSE.7 If initial screening with the Mini-Cog indicates dementia, then a full dementia work-up should be initiated. For reimbursement purposes, the diagnostic code for “Memory Loss” can be used until the work-up is completed. Once the diagnosis is confirmed, the appropriate code can then be recorded.
Remembering the Caregiver: The “Hidden Patient”
Primary care clinicians who treat patients with AD actually have two patients: the person with AD and the caregiver of the person with AD. The very early symptoms of AD, such as memory lapses and repetitive questioning, can be trying, but the neuropsychiatric symptoms such as verbal or physical abuse or combative behavior that may manifest as the disease becomes more entrenched can take a huge toll on the caregiver. Caregiving is a time- and labor-intensive job. Thus, providing care for a family member with AD can be a source of enormous stress. Stress, in turn, can contribute to mental and physical morbidity. It is well known that caregivers of patients with AD have a higher prevalence and incidence of depressive and anxiety disorders than non-caregivers.8
Caregivers are also at increased risk for physical illnesses. As compared with non-caregiver controls, caregivers of patients with AD—particularly older persons—are reported to have higher levels of D-dimer and interleukin-6, two markers of systemic inflammation and coagulation activation. These markers are linked to the frailty syndrome, a state of accelerated health deterioration and rapid aging leading to greater disease vulnerability, especially premature cardiovascular disease, and mortality.9 Caregivers of patients with AD are also less likely to engage in preventive health behaviors that might help ward off the more calamitous effects of chronic stress. Caregivers report that they lack adequate sleep, exercise, and time to visit their clinicians; they also report smoking and drinking more than usual, and taking a greater number of prescription medications.10
A study of 2477 caregivers found that caregivers had lower mental and physical scores on the SF-12® Health Survey (a multidimensional measure of health-related quality of life) than an age-adjusted normative sample.11 The variables linked to lower mental health scores in caregivers included patient depression, disruptive behavior, a recent emergency visit by the patient, and the number of hours devoted to caregiving. Worse physical health in the caregiver was associated with increased patient disruptive behavior and recent patient hospitalization.
The ill health effects linked to providing care for individuals with AD are more than somatization on the part of the caregiver. The demands of the caregiving role may cause caregivers to neglect their own health and suffer very real consequences of increased disease burden as a result. Consider the following two hypothetical cases. The first demonstrates how caregiving demands contribute to poor caregiver health.
Case 1
Mary is a 53-year-old woman with type 2 diabetes mellitus, a disorder that requires constant vigilance, a healthy diet, and an appropriate amount of exercise to be successfully controlled. Three years ago, her mother, now age 76 years, was diagnosed with probable AD; Mary has been her sole and constant caregiver since that time. Over the past year, Mary’s mother’s condition has worsened considerably. She is no longer able to dress or care for herself and has difficulty sleeping through the night. She has had arthritis for some time and lately her gait and mobility have been compromised. As a result, she is at increased risk for falls. She can now no longer be left alone. Mary is very worried about her own and her mother’s future. Before her mother became dependent upon her, Mary watched her diet and participated in frequent moderate exercise. Walks in her neighborhood provided her with not only physical activity but also an opportunity for socializing with neighbors. Since her mother now requires constant care and oversight, Mary is reluctant to leave the house. Also, as she has less time for herself and for managing her own needs, her eating habits have deteriorated. In the last six months, Mary has gained weight because of her poor diet and lack of exercise. She admits that she hasn’t been eating as well as she should. She feels burdened and isolated.
The second case illustrates how caregiver stress can contribute to or worsen anxiety and depression in any individual vulnerable to mood disorders.
Case 2
Francisco is a healthy 70-year-old man with a history of depression who is caring for his 68-year-old wife who has AD. Over the past few months, Francisco has uncharacteristically begun to complain of increased aches and pains. His family encouraged him to see his clinician because of their growing concern for his health. Since their insistence that he seek medical help began, he has been evaluated several times, but no cause for Francisco’s physical complaints has been found. Most recently, his son accompanied him on his medical appointment and told his father’s clinician that lately Francisco has had episodes of uncharacteristic impatience with his wife, and that he has begun berating and arguing with her. The son is concerned about the change in his father’s behavior.
These cases are examples of caregivers who are themselves in need of help, and should serve as reminders to clinicians to be attentive to the caregiver, and especially sensitive to any progression of chronic diseases such as diabetes, hypertension, and depression, or to the establishment of others such as stress ulcers or changes in personality and behavior—developments that might signal caregiver distress.
Maximizing Patient and Caregiver Health: Developing Appropriate Interventions
The caregiver tries to ensure the well-being of the patient with AD; therefore, clinicians must work to improve the health and well-being of the caregiver. To better serve the needs of caregivers of different ethnic and racial groups, researchers are investigating how caregiving differs in various cultures, and examining the factors that contribute to caregiver stress in these groups in order to develop relevant interventions. One important research finding is that people from different cultures may have different expectations of caregiving. In a sample of African-American (n = 76) and non-Hispanic white (n = 88) caregivers, a perceived lack of informal supports and a sense of incompetence worsened stress among African-American caregivers. Non-Hispanic white caregivers were predominantly affected by disruptive behavior and poor cognitive function. One potential explanation for the difference between the two groups is that expectations of filial responsibility tend to be stronger in the African-American community. When caregivers are unable to meet these expectations, they may become more vulnerable to stress.12
Racial differences also appear to affect utilization of skilled nursing facilities and home healthcare services. Using National Long-Term Care Survey data, researchers held screening interviews with African-American (n = 369) and non-Hispanic white (n = 2760) functionally impaired people (age 65 yr and older) living in the community to investigate how race affected use of these services, and to what extent family structure and social class explained any differences observed. They found that elderly African Americans make more use of these services at later ages than their non-Hispanic white counterparts, and that when children and grandchildren are involved, the use of these services is delayed until even later ages.
In addition, when formal assistance is required, African Americans are more likely than non-Hispanic white persons to use home healthcare over skilled nursing facility care. Social class has little influence on the risk differential. Also, contrary to what might be expected, African-American elderly persons do not offset their lower rate of skilled nursing facility use with a higher rate of home healthcare use.13 In addition to different culturally-derived expectations about caregiving, different groups may also have culturally influenced tendencies that lead to different coping strategies. A review of 12 studies published since 1985 that examined the effect of race, culture, and/or ethnicity on the experience of caregiving as it pertains to persons with dementia found the following: non-Hispanic white caregivers frequently used support groups and obtained assistance from professionals to help manage their responsibilities; African-American caregivers were more likely to turn to prayer, faith, or religion, and to discuss caregiving with members of the clergy and friends; and Hispanic-American and African-American caregivers were reported to rely more heavily on informal rather than formal support.6 It is very important to be aware of these cultural factors and the influence they exercise over various ethnic and racial groups.
Minimizing Caregiver Stress
Interventions That Improve Caregiver Well-Being
Studies have found that time-intensive interventions can be somewhat effective. A meta-analysis of caregiver intervention studies found positive effects on caregiver subjective well-being, caregiving ability, and knowledge about dementia symptoms across many types of caregiver interventions. Psychoeducational interventions that required the active participation (eg, role playing, applying new knowledge gained from dementia education presentations to individual problems) of caregivers were associated with the broadest effects.14 Likewise, a stress-coping intervention produced better scores than patient behavior management alone on caregiver general well-being and a trend toward decreased risk of depression, suggesting that brief primary care interventions may be effective in reducing caregiver distress and burden. Conversely, interventions that focus only on care recipient behavior, without addressing caregiving issues, may not be as adequate for reducing caregiver distress.15 These interventions are most effective in increasing caregiver knowledge and caregiving ability.16
The caregiver interventions examined in these studies are all time-intensive, and they may not be feasible or available for some office practices. Those unable to implement programs such as these in their communities should refer caregivers of persons with AD to respite services (if available in the community), provide them with educational materials to improve their knowledge about dementia and how to manage symptoms, and encourage them to join support groups for both emotional support and more information about AD. These efforts may work better if they are culturally appropriate. All caregivers should be referred to the Alzheimer’s Disease Education and Referral (ADEAR) Center: www.nia.nih.gov/Alzheimers/AlzheimersInformation/AboutUs.htm.
Patient Interventions with Donepezil, Rivastigmine, and Galantamine
Treating the symptoms of AD reduces caregiver workload and caregiver stress. ChEIs have demonstrated beneficial effects on caregiver well-being. The amount of time spent in caregiving has been shown to constitute a large component of caregiver burden, and maintaining patient function for a longer period can help alleviate this burden. In a 1-year, prospective, double-blind, randomized, placebo-controlled study, donepezil treatment reduced the amount of time caregivers spent assisting patients with mild-to-moderate AD as compared with placebo. As the condition of the patients deteriorated throughout the study, it was expected that caregiver time would increase. As anticipated, following 52 weeks, caregivers of placebo-treated patients (n = 94) were providing almost two hours (106.8 min) more care each day than at study baseline. However, for those caregivers of donepezil-treated patients (n = 96), their time burden had increased by only about 43 minutes each day. Caring time between the two groups, relative to baseline, was a little more than one hour (64.2 min) each day and was statistically significant (P = 0.03).17
Slowing disease progression also reduces caregiver stress. A randomized, double-blind, placebo-controlled study showed that caregivers of patients with moderate-to-severe AD treated with donepezil (n = 141) had mean total scores on the Caregiver Stress Scale at baseline that were similar to those of caregivers of placebo-treated patients (n = 149). By the 24th week, caregiver ratings favored donepezil-treated patients over placebo-treated patients (P < 0.005), with caregivers of donepezil-treated patients reporting the need to spend less time assisting with activities of daily living (ADL; a mean difference of about 1 hr/day).18 Overall, donepezil-treated patients showed a significantly slower rate of decline in instrumental ADL (IADL) and basic ADL than placebo-treated patients, and caregivers demonstrated lower levels of caregiver stress. Additionally, a 24-week, double-blind, randomized, placebo-controlled, withdrawal study was designed to measure the effects of donepezil on the treatment of neuropsychiatric symptoms and related caregiver distress in patients with mild-to-moderate AD with marked neuropsychiatric symptoms.19 After 12 weeks of open-label treatment, total neuropsychiatric symptoms and associated caregiver distress were lower with donepezil as compared with baseline (Neuropsychiatric Inventory [NPI], 22 vs 13 points, P < 0.0001; NPI-Caregiver Distress [NPI-D] Scale, 13.5 vs 7.9 points, P < 0.0001). These results suggest that in correlation with patients demonstrating significant improvements in various neuropsychiatric symptoms following treatment with donepezil, caregivers also showed significant improvement in their level of distress in relation to these symptoms.19
Recently, two 12-week, open-label studies evaluating the efficacy and safety of donepezil in minority populations were published. The first study confirmed the effectiveness of donepezil in African Americans with mild-to-moderate AD, demonstrating significant improvements in cognition, global function, and memory. Donepezil was also well tolerated.20 Although caregiver burden was not an efficacy measure in this study, previous studies have indicated that maintaining patient function for a longer period helps alleviate caregiver burden. The second study indicated cognitive improvement and safety results for donepezil in Hispanic patients with mild-to-moderate AD similar to those reported in the general population. Furthermore, a significant improvement was observed in the NPI-D Scale total score (P = 0.05), suggesting a positive impact on caregiver burden associated with patient behavior in this patient population.21 To date, these are the only studies in the literature reporting on treatment of AD in minority populations.
Rivastigmine has also been shown to be effective in alleviating caregiver burden. In a 6-month, prospective, open-label, observational study, approximately one-half of caregivers of patients with mild-to-moderate AD reported no increase in burden, and approximately 25% reported improvement.22 Patients in this study were either ChEI-naϊve (n = 1869) or had switched to rivastigmine from another ChEI at the start of the study (n = 749). In a second prospective, observational study involving only rivastigmine-naϊve patients with mild-to-moderate AD (n = 175), caregivers reported less burden and better general health. After patients were treated for 6 ± 1.5 months with rivastigmine, caregivers demonstrated statistically significant improvements in both the Zarit Caregiver Burden Scale (P = 0.036) and the 12-item version of the General Health Questionnaire (P = 0.029). However, caregivers’ IADL scores and time spent caring did not change over the course of the study.23 Another observational study involving rivastigmine demonstrated a significant relationship between disease severity and time spent caregiving. These findings were used to estimate reduced caregiver burden resulting from delay in disease progression following treatment with rivastigmine. Results suggested that over a two-year period, delay in disease progression could reduce caregiving time by approximately 691 hours for caregivers of patients with mild AD.24
Galantamine has also been found to be effective in reducing the amount of time caregivers must allot to caring for the patient with AD. In a 12-week, open-label study testing the effects of galantamine on attention in patients with mild-to-moderate AD (n = 373), galantamine improved caregiver stress and time spent caring for patients from baseline to end point.25 Data pooled from two concurrent, double-blind, randomized, placebo-controlled, 6-month trials with patients with mild-to-moderate AD showed that caregivers of galantamine-treated patients (n = 411) spent approximately 30 minutes less per day (P = 0.011) assisting patients with ADL than caregivers of patients given placebo (n = 414). Furthermore, among patients with moderate AD, caregivers of galantamine-treated patients reported a mean daily time savings of 53 minutes (P = 0.021). Caregivers of galantamine-treated patients also reported changes in the time that patients could be left unattended, with a mean daily savings of 27 minutes.26 In a secondary analysis of a double-blind, placebo-controlled, parallel-group trial of patients with mild-to-moderate AD treated with galantamine, alterations in caregiver distress were measured by the NPI-D scale. High-dose galantamine (n = 273) was associated with a significant reduction in caregiver distress concomitant with lower levels of behavioral disturbance as compared with placebo (n = 286).27 A significant reduction was also observed in the total NPI caregiver burden (P < 0.05) in a three-month, open-label, multicenter study designed to assess the impact of galantamine on behavioral disturbances and associated caregiver burden in noninstitutionalized patients with mild-to-moderate AD (n = 124).28
No studies have been published regarding the impact of memantine therapy on caregiver stress.
Conclusions
AD is especially prevalent, underdiagnosed, and undertreated in African-American and Hispanic-American populations. All patients age 65 years and older should be routinely screened for the disorder, and physicians should be especially alert to its occurrence in minority groups, as caregivers have been shown to interpret early symptoms of the disease as normal aging.
Caregiver support is an important aspect of providing care for patients with AD. Caregivers from different ethnic/racial groups may have different needs and/or methods of dealing with the stress of caregiving. Not all ethnic and racial groups respond to particular stressors in the same way. Greater understanding can result in more effective caregiver interventions. A better understanding of those cultural characteristics that may affect or influence coping strategies can help physicians to tailor interventions appropriately to meet the particular unique needs of caregivers of patients with AD.
Successful management of AD can reduce caregiver burden. According to the Alzheimer’s Association, active management of AD, including currently available treatment options, can significantly improve quality of life through all stages of the disease for both the patient with AD and his or her caregiver.1 It should be noted, however, that Britain’s National Institute for Health and Clinical Excellence (NICE) has recently issued guidance that restricts the use of ChEIs and memantine in general for the treatment of AD in their National Health Service.29
Furthermore, the American Academy of Family Physicians suggests that the physical and emotional health of the caregiver is essential to achieve optimal care of the patient with AD.30 Thus, pharmacologic and other treatment should be considered and instituted as early as possible to increase the potential to maintain patient function for a longer period and slow symptom progression. Intervention strategies designed to support the caregiver and early medical treatment of patients with AD can help to reduce the progression of AD symptoms. Together they help maintain patient function and ease caregiver burden.
Family members should be encouraged to become treatment advocates by bringing cognitive and functional changes to the physician’s attention as soon as they are recognized.
Dr. Griffith has received speaker honoraria from Eisai Inc. and Pfizer Inc, and was a paid consultant to Eisai Inc. and Pfizer Inc in connection with the development of this manuscript. Editorial support was provided by W. Watkins, MS, of PAREXEL, and was funded by Eisai Inc. and Pfizer Inc.
Acknowledgment
This article was supported in part by the Clinical Research Center of Meharry Medical College, grant # P20RR011792 from the National Institutes of Health and RCMI Clinical Research Infrastructure Initiative. Dr. Griffith is Professor of Clinical Medicine (Neurology), Chief, Division of Neurology, Department of Internal Medicine, and Program Director, Stroke Prevention/Intervention Research Program (SPIRP), Morehouse School of Medicine, Atlanta, GA.