
A Toddler With an Unusual Presentation of Hemophilia A
A previously healthy 18-month-old boy presented to the emergency department (ED) with a chief complaint of a 1-day history of refusal to bear weight on his left foot. The parents stated that the condition had been acute in onset, with no associated trauma, fever, or respiratory illness. Upon presentation, he was afebrile, his vital signs were within normal limits, and physical examination finding were unremarkable. Radiographs of the left lower extremity (including the pelvis, femur, tibia, fibula, and foot) were negative for fractures or dislocations. He was discharged home on ibuprofen.
The child returned to the ED within 48 hours with the same complaints. This time, a low-grade fever was noted, with the rest of his vital signs within normal limits. Now, physical examination findings were significant for mild swelling (without erythema or warmth) of the left foot, 3 bruises over the flexor surface of the left ankle, mild tenderness to palpation, and decreased range of motion.
Results of laboratory tests (complete blood count, chemistry panel, urinalysis, antistreptolysin O titer, C-reactive protein test) were all unremarkable, except for a mildly elevated erythrocyte sedimentation rate of 14 mm/h. Magnetic resonance imaging (MRI) and ultrasonography scans were negative for hemarthrosis, although MRI revealed nonspecific findings of soft tissue swelling of the distal left lower extremity (Figures 1 and 2). Upon admission, a family history of hemophilia was elicited; of note, the patient had been circumcised at birth without significant bleeding. Results of coagulation studies showed a prolonged partial thromboplastin time of 67.2 seconds and low factor VIII level (18%). He was started on antibiotics for suspected cellulitis, and a second factor VIII assay showed a level of 1%.
The patient received a diagnosis of hemophilia A and was managed with factor VIII replacement therapy, with great improvement of his symptoms. He remained afebrile throughout the remainder of the hospital course, with normal activity at the time of discharge.
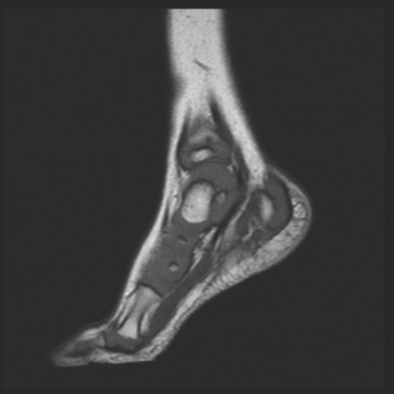
Figure 1. Magnetic resonance imaging scans revealed nonspecific findings of soft tissue swelling of the distal left lower extremity in an 18-month-old boy.
Discussion
Hemophilia A is caused by a deficiency in plasma of coagulation factor VIII. It is the most common X-linked inherited bleeding disorder and is characterized by hemorrhages in the joints and soft tissue.3 Approximately one-third of newly diagnosed infants or young children have no family history of hemophilia, and the disorder may be a result of a spontaneous mutation in the F8 gene, which encodes factor VIII.1
Bleeding is the hallmark of hemophilia; however, the site and pattern of the bleeding vary over the lifetime of the patient. In newborns, hemophilia more frequently manifests as intracerebral and extracerebral hemorrhages and bleeding from circumcision or venipuncture.1 While uncommon in newborns, joint and soft tissue hemorrhages become more evident as a child grows and as mobility increases. Hemarthrosis manifests in the ankles in a toddler as he or she learns to walk (usually before the age of 2 years) and then the knee and hip as the child grows older.1
Repeated joint bleeds lead to chronic synovitis, bony changes, and, eventually, marked joint dysfunction (eg, reduced range of motion, stiffness, instability, swelling, pain). In growing children, synovitis also causes hypertrophy of the epiphyseal growth plates, potentially leading to bony hypertrophy, leg-length discrepancy, and angular deformities. The musculoskeletal dysfunction and associated pain affect children’s quality of life and lead to restrictions in activities, including school, social participation, and normal activities of daily living.2
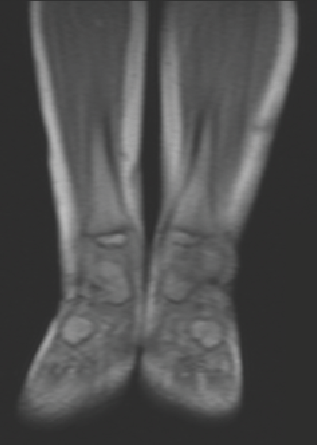
Figure 2. MRI revealed nonspecific findings of soft tissue swelling of an 18-month-old boy’s distal left lower extremity.
If synovitis occurs, treatment is required. Options include factor VIII replacement at the time of bleeding, splinting, and physiotherapy. Other treatments include chemical synovectomy, radiosynovectomy with or without intra-articular corticosteroids; arthroscopic or open synovectomy, and joint arthroplasty.2
Prevention of bleeding is the key to ensuring the best musculoskeletal outcome in patients with hemophilia, and this can be achieved with early prophylactic administration of factor concentrates.3 The goal of primary prophylaxis (started before onset of joint damage) is preventing recurrent bleeds and the development of chronic arthropathy.1,3 Secondary prophylaxis (started after onset of joint damage) generally appears to be unable to reverse all existing or developing joint damage. Nevertheless, numerous studies have shown that even secondary prophylaxis can reduce bleeding, retard joint deterioration, help prevent hospitalization and missed school days, improve physical function, reduce pain, and enhance quality of life.2
In patients with no previous history of bleeding or with an unremarkable family history, a diagnosis of hemophilia can be easily overlooked. If it is not properly managed, hemophilia A can lead to chronic disease and lifelong disabilities. Awareness of its clinical manifestations, including unusual presentations,4 is crucial in implementing appropriate management and preventive strategies in order to minimize physical deformity, chronic pain, and negative effects on a person’s health-related quality of life.
References:
1.Kulkarni R, Soucie JM. Pediatric hemophilia: a review. Semin Thromb Hemost. 2011;37(7):737-744.
2.Sherry DD. Avoiding the impact of musculoskeletal pain on quality of life in children with hemophilia. Orthop Nurs. 2008;27(2):103-110.
3.Zimmerman B, Valentino LA. Hemophilia: in review. Pediatr Rev. 2013; 34(7):289-295.
4.Sakurai Y, Sugimoto H, Yoshida K, et al. Superficial fibromatosis mimicking subcutaneous hematoma: an unusual and difficult diagnosis in a patient with mild hemophilia A. Int J Hematol. 2007;85(1):1-4.
Dr Trifonova and Dr Jean are second-year pediatrics residents, Dr Fernandes and Dr Castellanos are third-year pediatrics residents, and Dr Mendez is director of the pediatrics residency program, all at Lincoln Medical and Mental Health Center in Bronx, New York.