
A 15-year-old girl was brought to the emergency department because of bilateral shoulder and hip pain associated with myalgia and fatigue. The symptoms had been present for 2 months and had increased in intensity over the past few days. The patient had systemic lupus erythematosus, asthma, and seizure disorder.
The patient appeared uncomfortable on examination. Temperature was 38°C (100.4°F); heart rate, 103 beats per minute; blood pressure, 114/62 mm Hg; and respiration rate, 22 breaths per minute. Diffuse tenderness was noted on palpation of the shoulders, hips, and muscles. There was no erythema, warmth, or swelling.
_________________________________________________________________________________________________________________________________________
Related Content
Toxic Epidermal Necrolysis: Overview of a Serious Skin Condition
Toxic Epidermal Necrolysis
_________________________________________________________________________________________________________________________________________
The white blood cell count was 2.9 3 103/µL (with 32% neutrophils, 28% bands, 30% lymphocytes, and 6% mononuclear cells); hemoglobin level, 11.6 g/dL; hematocrit, 35.4%; and platelet count, 160 3 103/µL. Other laboratory findings included sodium, 132 mEq/L; potassium, 4.2 mEq/L; chloride, 20 mEq/L; total calcium, 7.7 mg/dL (a second calcium measurement was normal); bicarbonate, 20 mEq/L; glucose, 105 mg/dL; urea( nitrogen, 8 mg/dL; and creatinine, 0.8 mg/dL. Results of a urinalysis were normal.
A screen for antinuclear antibodies was positive (titers greater than 1:160). Anticentromere antibody test results were negative, anti-dsDNA titers were 25.75 IU (normal, less than 25 IU); anti-Smith antibody titers and anti-ribonucleoprotein titers were both normal (less than 20 U). C3 and C4 complement levels and the erythrocyte sedimentation rate were normal. The C-reactive protein level was 0.12 mg/dL (normal, less than 0.8 mg/dL). Creatine kinase and aldolase levels were 1701 U/L (normal, 26 to 140 U/L) and 15.4 U/L (normal, 1.0 to 7.5 U/L), respectively. Results of a serum cold agglutinin test were negative.
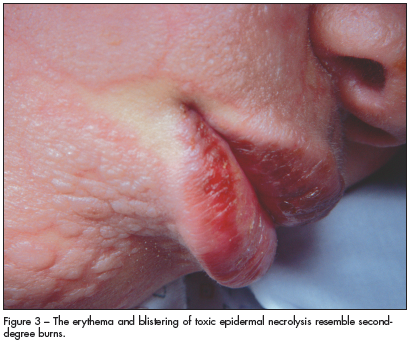
Thirty-six hours after admission, a high-grade fever developed and an erythematous, vesicular rash erupted on the patient's face (Figures 1, 2). The rash quickly spread to her neck and chest and progressed to flaccid bullae (Figure 3).
Because the rash and laboratory findings were not typical of a lupus flare, a dermatologist was consulted, and a skin biopsy was obtained. Histological examination revealed full-thickness epidermal necrosis, consistent with toxic epidermal necrolysis (TEN).
On further questioning, it was learned that 2 months before presentation, the patient had started taking lamotrigine(. This agent is among those associated with the anticonvulsant hypersensitivity syndrome (discussed on the next page).1 The patient was also taking beclomethasone and albuterol, which are not associated with TEN.
Infliximab infusion therapy was started based on the recommendation of the allergy and immunology service, and lamotrigine was discontinued. Infliximab( was considered the better choice over intravenous immunoglobulin (IVIG) because of its faster clinical effect. After a few hours of treatment, the skin lesions stopped progressing and no new lesions were noted. The patient remained hemodynamically stable until discharge. During her hospital stay, an electroencephalogram revealed no seizure-like activity. A neurological follow-up appointment was scheduled for further evaluation before the patient started taking another anticonvulsant medication.
DIFFERENTIAL DIAGNOSIS OF VESICULOBULLOUS LESIONS Many diseases are characterized by vesiculobullous lesions. The cause varies, as does the age at onset and pattern. Erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and TEN are a group of exfoliative diseases of the skin and mucous membranes. It has been suggested that SJS and TEN share enough clinical and microscopical features to classify them as end points of the same spectrum. In fact, these conditions often are considered the same disease entity, differing only in the extent of the involved area. SJS affects less than 10% of the total body surface, whereas TEN affects more than 30%. This leaves a zone of overlap between 10% and 30%, referred to as SJS/TEN with ocular involvement and stomatitis.
Many diseases are characterized by vesiculobullous lesions. The cause varies, as does the age at onset and pattern. Erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and TEN are a group of exfoliative diseases of the skin and mucous membranes. It has been suggested that SJS and TEN share enough clinical and microscopical features to classify them as end points of the same spectrum. In fact, these conditions often are considered the same disease entity, differing only in the extent of the involved area. SJS affects less than 10% of the total body surface, whereas TEN affects more than 30%. This leaves a zone of overlap between 10% and 30%, referred to as SJS/TEN with ocular involvement and stomatitis.
Pediatric conditions that may resemble SJS by their mucocutane- ous involvement include Kawasaki disease; staphylococcal scalded skin syndrome, in which the blister cleavage plane is intraepidermal; collagen vascular diseases; serum sickness; graft versus host disease; chemical burns; drug eruptions; and pemphigus.2
THE CAUSE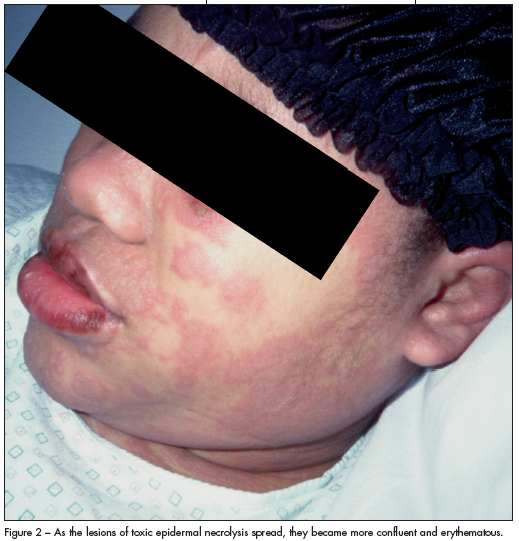 TEN and SJS seem to be caused by immunological reactions to foreign antigens. Drugs have been implicated in 77% to 94% of cases.3 Anticonvulsants (phenobarbital, carbamazepine(, oxcarbazepine(, phenytoin, and lamotrigine) were the trigger in half of these cases. Antibiotics, including penicillin, sulfa drugs, cotrimoxazole, cefuroxime, and vancomycin(, were the second most commonly implicated drug class. Acetaminophen was the trigger in a few cases.3 Allopurinol( is a common cause of SJS/TEN in adults.
TEN and SJS seem to be caused by immunological reactions to foreign antigens. Drugs have been implicated in 77% to 94% of cases.3 Anticonvulsants (phenobarbital, carbamazepine(, oxcarbazepine(, phenytoin, and lamotrigine) were the trigger in half of these cases. Antibiotics, including penicillin, sulfa drugs, cotrimoxazole, cefuroxime, and vancomycin(, were the second most commonly implicated drug class. Acetaminophen was the trigger in a few cases.3 Allopurinol( is a common cause of SJS/TEN in adults.
Anticonvulsant hypersensitivity syndrome is defined by the triad of fever, rash, and symptomatic or asymptomatic internal organ involvement, including primarily hepatitis, nephritis, and lymphadenopathy. The mucocutaneous eruption appears about 4 weeks to 3 months after starting certain anticonvulsants and may be similar to that of EM, SJS, or TEN.4
The pathogenesis of TEN, although unproved, may involve a hypersensitivity phenomenon that results in damage primarily to the basal cell layer of the epidermis. Epidermal damage appears to result from Fas (CD95)-mediated keratinocyte apoptosis. Other triggers of SJS and TEN may include infection, neoplasia, radiation therapy, sunlight, and pregnancy.
CLINICAL CHARACTERISTICS OF TENTEN, or Lyell syndrome, is defined by the following characteristics:
•Widespread blister formation and morbilliform or confluent erythema, associated with skin tenderness.
•The absence of target lesions.
•Sudden onset and generalization within 24 to 48 hours.
•Full-thickness epidermal necrosis with minimal or absent dermal infiltrate.
 The prodrome usually consists of fever, malaise, localized skin tenderness, and diffuse erythema. Inflammation of the eyelids, conjunctivae, mouth, and genitals may precede skin lesions. Flaccid bullae may develop. The hallmark of TEN is the sloughing of the skin to a raw, oozing state after the blisters rupture. The skin separation occurs at the dermoepidermal junction and, even in unblistered areas, the epidermis can be removed easily by light tangential pressure (the Nikolski sign). TENis exceedingly rare in infants younger than 6 months.
The prodrome usually consists of fever, malaise, localized skin tenderness, and diffuse erythema. Inflammation of the eyelids, conjunctivae, mouth, and genitals may precede skin lesions. Flaccid bullae may develop. The hallmark of TEN is the sloughing of the skin to a raw, oozing state after the blisters rupture. The skin separation occurs at the dermoepidermal junction and, even in unblistered areas, the epidermis can be removed easily by light tangential pressure (the Nikolski sign). TENis exceedingly rare in infants younger than 6 months.
This patient's presentation was atypical of TEN. A lupus flare-up was considered initially because she had been previously hospitalized for elevated muscle enzyme levels, which were managed with intravenous hydration. The working diagnosis at that time was lupus-related myositis/dermatomyositis, but it was not finalized. At discharge, the muscle enzyme levels remained elevated; however, the rash had resolved completely. She will continue to be monitored.
TREATMENT AND PROGNOSISThe management of SJS and TEN includes immediate hospitalization. Patients with TEN are best treated in a burn unit, if available. The optimal treatment of TEN is controversial. Supportive therapy is the standard of care for SJS/TEN and includes close monitoring of fluid and electrolyte status, nutritional support, meticulous wound care, and control of pain and infection.5 Prompt withdrawal of the suspected causative agent(s) may decrease mortality.
IVIG, which blocks the Fas receptor, may be an effective treatment. In one study, cessation of cutaneous blistering was observed in all patients within an average of 2 days (range, 1 to 3 days) after IVIG was started and 3.75 days (range, 1 to 10 days) after blister onset.6
Systemic corticosteroids have been used with or without IVIG. Patients treated with IVIG without corticosteroids at an average dose had a more rapid clinical response than patients who received IVIG with corticosteroids.6 There have been reports of increased mortality with the use of corticosteroids in severe exfoliating cases, because the risk of infectious complications increases with corticosteroid-induced immunosuppression.7
Immunomodulators have been effective in patients with TEN. Studies have shown tissue sections before anti-tumor necrosis factor a (TNF-a) therapy with strong immunoreactivity for TNF-a in the keratinocytes of the outer necrobiotic parts of the epidermis and also in scattered basal and suprabasal keratinocytes. TNF-a was also strongly expressed in perivascular inflammatory cells in the dermis and in inflammatory cells infiltrating the epidermis.8 In one case, epidermal detachment stopped within 24 hours, and after 5 days, re-epithelialization was almost complete.7 This is clearly faster than the reported clinical response time after starting IVIG. Infliximab binds to soluble and membrane-bound TNF-a and, in addition, induces apoptosis of TNF-a-producing cells--especially of activated T cells. This agent has been used to treat other inflammatory conditions as well.7
KEY POINTS FOR YOUR PRACTICEDifferences between SJS and TEN include mortality risk and the extent of epidermal detachment. Poor prognosis has been linked to advanced age, ingestion of many different kinds of drugs, idiopathic onset, respiratory failure, and laboratory abnormalities (such as decreased renal function, hyperglycemia, neutropenia, lymphopenia, and thrombocytopenia). Complications with secondary infection and sepsis are frequent in TEN.9
Research on the SJS/TEN spectrum has primarily involved adults. In children, most cases of SJS can be traced to an infectious agent; TEN is almost exclusively drug-related in both children and adults. Therefore, a careful history of previous and current medications is crucial. *