
Two Girls With Short Stature
CASE 1
A 14-year-old white girl whose menstrual periods have not begun presents with concerns that many of her peers are already menstruating.
The patient weighs 50 kg (110 lb, 50th percentile) and is 58.5 in tall (third percentile). She was 49 in at age 10 and 54 in at age 12. Her father is 5 ft 7.5 in tall (25th percentile) and her mother is 5 ft 2.5 in tall (25th percentile).
The patient’s blood pressure is 100/60 mm Hg. She is in Tanner stage 2 for breast and pubic hair development and has normal female external genitalia. Physical findings and past medical history are unremarkable.
The patient has a normal hemogram, normal thyroid function, and normal bone age. Levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) are slightly elevated; estradiol levels are low. Definitive diagnosis is made by chromosome analysis. Karyotyping shows 46,XX/45,X.
CASE 2
A 7-year-old African American girl sees her pediatrician because she is considerably shorter than her peers. She was born at 41 weeks’ gestation after an uncomplicated pregnancy and had a normal postnatal course. She weighed 3.42 kg (7.5 lb)at birth (50th percentile) and was 18.7 in long (30th percentile). Her past medical and family histories are unremarkable.
She now weighs 24 kg (53 lb, 60th percentile) and is 42 in tall (below the fifth percentile). She previously measured 36 in at 4 years and 39 in at 6 years. Her father is 6 ft tall (75th to 90th percentile), her mother is 5 ft 5 in tall (50th to 75th percentile), and her 5-year-old sister is 41 in tall (50th to 75th percentile). Midparental height is 66 in (calculated by adding the mother’s height to the father’s height and dividing by 2, then subtracting 2.5 in for girls).

Aside from short stature, physical examination findings are normal. The patient is in Tanner stage 1, with normal female external genitalia. She also has a normal hemogram, normal thyroid function, and normal bone age. Karyotyping shows 45,XO. Growth charts for the patients in both cases are shown here (Figure 1).
WHAT IS THE DIAGNOSIS—
AND WHAT ARE THE
TREATMENT OPTIONS?
ANSWER:
TURNER SYNDROME
Both patients presented with short stature; the first also had primary amenorrhea. In both cases, physical findings were unremarkable except for short stature. Thus, a normal physical examination does not rule out Turner syndrome (TS).
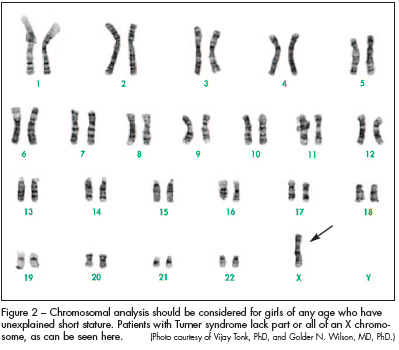
Although in recent years TS is often recognized in utero, many patients with mosaicism do not have the “classic” features of this disorder— and the diagnosis might therefore be easily missed until pubertal years when the patient is amenorrheic (as with the patient in case 1). Therefore, chromosomal analysis should be considered for girls of any age who have unexplained short stature (Figure 2). Early diagnosis is crucial for appropriate treatment and counseling.
Patients with TS lack part or all of an X chromosome. The most common sex chromosome abnormality in females, TS occurs in approximately 50 per 100,000 liveborn girls.1 Roughly 10% of spontaneously aborted fetuses have this disorder, and the incidence has been estimated to be 0.8% in zygotes. As such, it may be the most common chromosomal disorder in humans.2 It appears that only about 1% of human 45,X zygotes survive to term, and those who do typically have a characteristic set of somatic abnormalities.1,2
GENETICS
TS can develop from the following mechanisms:
- X chromosome monosomy, which is associated with a loss of the whole X chromosome.
- X chromosome mosaicism, in which a sex chromosome may also be lost during early stages of embryonic
- development, such that only some cells receive a single X chromosome.
- X chromosome defects, such as fragmented or deleted portions and ring formation.
Short stature homeobox (SHOX) is a transcription factor that plays a particularly important role in the growth and maturation of bones in the arms and legs. One copy of the SHOX gene is located on each of the sex chromosomes (the X and Y chromosomes) in the pseudoautosomal region.3 Females with TS have only 1 copy of the SHOX gene instead of the usual 2 copies; this reduces the amount of SHOX protein by half. Researchers believe that this deficiency is at least partly responsible for short stature and skeletal abnormalities (such as unusual rotation of the wrist and elbow joints) in females with this condition.3
CLINICAL PRESENTATION
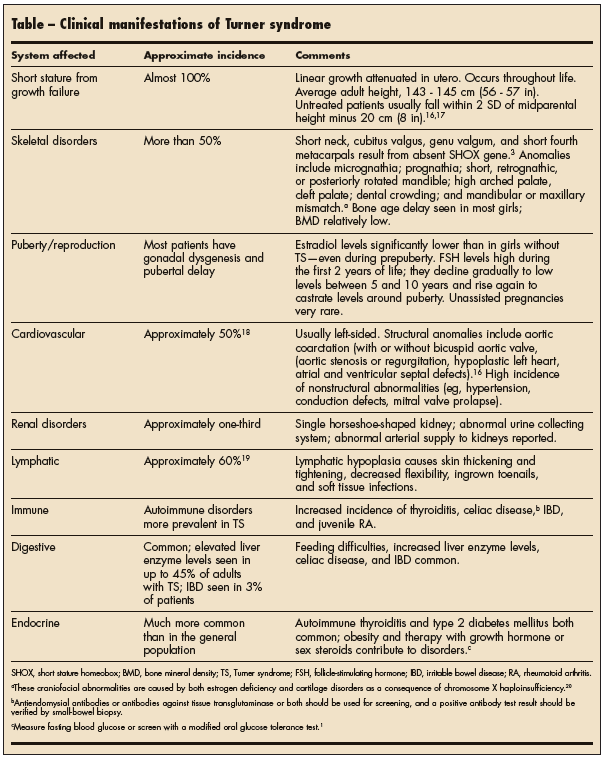
The common clinical presentations of TS are short stature, lymphedema of the hands and feet (Figure 3), a broad chest with widely spaced nipples, a low hairline, low-set ears, cubitus valgus, webbed neck (Figure 4), and amenorrhea. The Table describes the myriad manifestations.
PSYCHOLOGICAL ANDEDUCATIONAL ISSUES
Patients with TS generally have normal intelligence. The exception is the rare patient with a tiny X-ring chromosome, who may present with severe mental retardation. TS patients may have problems with visuospatial organization (eg, difficulty in driving), deficits in social cognition, trouble with nonverbal problem-solving tasks (eg, math problems), psychomotor deficits (such as clumsiness), and attention-deficit disorder.4,5 The neurodevelopmental abnormality may result fromthe X-chromosome monosomy or from hormonal deficiencies associated with gonadal dysgenesis.5 It is compatible with right cerebral dysfunction, and the deficits generally involve nonverbal skills.


MANAGEMENT
Multispecialty team management is crucial for girls with TS. The primary care pediatrician orchestrates the team.6
Growth hormone (GH). GH is being used successfully to treat girls with short stature. The earlier the GH therapy is initiated and the higher the dosage, the more robust the response is.7 The goal of the therapy is to attain a normal height for age as soon as possible; growth should progress through puberty so that the patient attains a normal adult height.7 Although GH can increase the patient’s adult height, many factors influence this, including8-10:
- The patient’s height and age at initiation of therapy.
- The duration and dosage of therapy.
- Concurrent treatment with anabolic steroids.
- The timing of estrogen replacement therapy.
For a young girl of normal height, GH therapy should be initiated at the FDA-approved dosage of 0.054 mg/kg/d. Levels of insulin-like growth factor (IGF-1) should be kept below 2 SD above the mean. For an older girl who is short, consider giving 0.067 mg/kg/d and increasing the dosage to 0.1 mg/kg/d to provide catch-up growth, regardless of the IGF-1 level.7,9
Anabolic steroids. Oxandrolone is the preferred androgen because it cannot be aromatized. It is also unlikely to produce virilizing effects or advancement in bone age at low dosage. When used alone, anabolic steroids increase short-term growth velocity but do not appear to improve the final height. Oxandrolone, in combination with GH, augments growth.9,11
Estrogen. Estrogens are important in the development of secondary sex characteristics and maintenance of the female reproductive system.12 They also cause growth and development of the uterus, fallopian tubes, and vagina. Along with other hormones, they cause enlargement of the breasts through promotion of ductal growth, stromal development, and the accretion of fat.
The timing of estrogen therapy is important. The longer the duration of estrogen-free GH treatment, the greater the final height attained. In one study, growth was stimulated for approximately 2 years after the initiation of estrogen therapy but then declined as bone age advanced.12 It was found that girls whose estrogen therapy was delayed until 15 years of age gained more height.12
SCREENING RECOMMENDATIONS
All patients with TS should have a baseline cardiovascularevaluation at the time of diagnosis. Females with a normal echocardiogram should undergo imaging every 5 years to rule out aortic root dilation. Those with abnormal echocardiographic findings need to be followed more frequently by the cardiologist. Aortic dissection must be considered in any TS patient with severe chest pain, and MRI scans should be obtained urgently.13-15
Routine screening with ultrasonography for renal abnormalities is also indicated for patients with TS.13-15 If results are abnormal, refer the patient for evaluation and therapy. Urinary tract infections should be treated vigorously and renal obstruction (if any) must be promptly
relieved.
 Psychological assessment should also be part of the treatment plan for each child with TS. Evaluation of intellectual, learning, and motor skills as well as social maturity is recommended before the child is enrolled in preschool programs. If cognitive strengths and weaknesses are identified, preventive and intervention strategies can be helpful. The adjuvant role of pubertal estrogen replacement on cognitive function remains unclear.
Psychological assessment should also be part of the treatment plan for each child with TS. Evaluation of intellectual, learning, and motor skills as well as social maturity is recommended before the child is enrolled in preschool programs. If cognitive strengths and weaknesses are identified, preventive and intervention strategies can be helpful. The adjuvant role of pubertal estrogen replacement on cognitive function remains unclear.
Many couples choose to adopt. Ovarian tissue and preservation of oocytes might be a possibility for future fertility treatments in patients with TS. The pregnancy rate achieved by embryo transfer in women with TS is similar to that of other oocyte recipients with primary ovarian failure.