
Vitamin B12: Considerations for Maintaining Optimum Health in Elders
This is the second article in a continuing series on nutrition in the elderly. The first article in the series,“Vitamin D and Calcium: Implications for Healthy Aging,” was published in the December 2011 issue of Clinical Geriatrics and can be found online at www.clinicalgeriatrics.com/articles/Vitamin-D-and-Calcium-Implications-Healthy-Aging. Future articles will discuss popular diets and nutritional assessment of the geriatric patient.
________________________________________________________________________________________________
Vitamin B12, a cobalt-containing, water-soluble compound, is one of eight naturally occurring B vitamins and is essential for maintaining normal hematologic and nervous system functions. Also known as cobalamin (Cbl), vitamin B12 is obtainable only from supplements, fortified foods, and proteins of animal origin, such as red meat, poultry, eggs, and dairy products. Dietary vitamin B12 from eggs has long been thought to have poor bioavailability, although this is currently the subject of an ongoing study by the US Department of Agriculture.1
In the United States, the recommended dietary allowance (RDA) of Cbl for men and women 50 years and older is 2.4 µg daily.2 The prevalence of Cbl deficiency, when defined as a serum or plasma concentration <148 pmol/L (200 pg/mL), increases with age and is estimated to affect 6% of adults 60 years and older.3 Combining serum levels with other markers, the Framingham study found that at least 12% of community-dwelling elderly adults have Cbl deficiency.4 Deficiency rates of 20% have been reported3 when older adults with subclinical vitamin B12 deficiency (asymptomatic with a borderline serum B12 level and/or elevated homocysteine [Hcy] or methylmalonic acid [MMA] levels5) are included.
The road to discovering vitamin B12 began with George Richards Minot and William Murphy,6 who were investigating liver extracts as therapy for pernicious anemia, an autoimmune disease that leaves the digestive track unable to absorb vitamin B12 from food.7 Prior to the researchers’ 1926 breakthrough, pernicious anemia was a fatal disease that affected nearly 50,000 individuals annually in the United States.7 Building on the work of Minot and Murphy, investigators Mary Shaw Shorb (whose father died of pernicious anemia) and Karl Folkers isolated the liver compound that came to be known as vitamin B12 in 1947. Merck and Company isolated vitamin B12 in crystalline form and subsequently demonstrated the compound’s efficacy as a treatment for pernicious anemia. We describe additional causes and possible effects of insufficient Cbl levels in older adults and discuss how to manage Cbl deficiency.
The Physiological Role of Vitamin B12
Vitamin B12, or Cbl, is essential for the production of S-adenosylmethionine (SAMe), a methyl donor for DNA, RNA, hormone, lipid, and protein synthesis.8 In addition to the association between Cbl deficiency and pernicious anemia, data have implicated insufficient Cbl intake or absorption in a number of neurological, psychological, and biological conditions, including neuropathy, dementia, depression, bone loss, and possibly stroke.9 Serum folic acid levels appear closely tied to Cbl insufficiency or deficiency, although the exact nature of the relationship between these B vitamins is not fully understood.8,10
Cbl, Folate, and Neurological Function
Cbl and folate are fundamental for maintaining normal central nervous system function. The association between Cbl deficiency and impaired cognition in older adults has been well described, with even otherwise healthy elderly adults showing evidence of cognitive impairment when serum levels of Cbl are low. Neurological disorders due to vitamin B12 deficiency occur in both sexes and typically peak between 60 and 70 years of age.10 The exact mechanism behind this relationship is unclear, but studies have show that Cbl and folate are especially important in neurotransmitter synthesis and in maintaining the health of myelin and glial cells. Sufficient quantities of Cbl and folate are required to metabolize Hcy, an intermediary amino acid involved in the synthesis of methionine. Methionine is an amino acid that serves as a building block of SAMe8 and is essential in nucleotide synthesis, genomic methylation, and nongenomic methylation.10 Excess circulating Hcy or its metabolites have been linked to neuron damage and vascular disease, both of which are major contributors to the development of dementia.11 It is clear that an increase in circulating Hcy is associated with cognitive decline and psychiatric disturbances, such as dementia. Although Hcy levels are sometimes elevated in patients without Cbl and folic acid deficiencies, these states are typically observed concomitantly.11-14
In a meta-analysis of 75 studies investigating Cbl deficiency, Hcy, and dementia, Werder concluded there was convincing evidence to suggest hyperhomocysteinemia was a risk factor for dementia and that this link was stronger than the one between low Cbl levels and dementia.13 Hassan and colleagues12 identified elevated plasma Hcy as an independent vascular risk factor for Alzheimer’s dementia and vascular dementia.
A more recent study by Tangney and associates14 evaluating vitamin B12 levels and Hcy levels in 121 community-dwelling elders (median age, 78.7±5.7 years) reported that global cognitive scores declined by 0.03 standardized units and white matter hyperintensity volume increased for each 1 µmol/L increase in Hcy concentration (P=.04).The authors also found that higher levels of MMA accumulation, another marker of vitamin B12 deficiency, correlated with lower episodic memory scores, reduced perceptual speed, and less total brain volume, which led them to conclude that low levels of vitamin B12 affect the brain via multiple mechanisms.14
Morris and associates11 analyzed nutritional data for 1684 participants (≥60 years of age) in the 1999-2002 US National Health and Nutrition Examination Survey (NHANES) and concluded that the relationship between Cbl and folate levels was significant in predicting the risk of cognitive impairment.Among individuals with low vitamin B12 levels, those who had high serum folate levels had a higher risk of cognitive impairment and anemia compared with those whose serum folate levels were in the normal range. Individuals with normal vitamin B12 status and high serum folate levels had the lowest rate of cognitive impairment. The authors hypothesized that the benefits of these nutrients may be tied to their contribution to Hcy remethylation.11
Even having levels of Cbl or folate considered normal by today’s standards might not be sufficiently protective against cognitive decline. Studies have associated Cbl and folate levels at the lower end of normal with abnormal effects and cognitive impairment in psychiatric patients and in otherwise normal healthy older adults.15 These individuals may lack the classical signs of Cbl and folate deficiency, namely peripheral neuropathy and macrocytic anemia.15 For example, Morris and colleagues found that 3% of elderly NHANES participants had Cbl concentrations <148 pmol/L, yet 4% of patients had macrocytic anemia. The remaining patients were among the 25% of participants who met the study’s definition of “low” vitamin B12, which used a serum MMA level >210 nmol/L as an alternative measure of Cbl status.11
A recent post-hoc analysis16 from a randomized, placebo-controlled trial that included individuals 70 years and older with mild cognitive impairment found that those who were randomly assigned to receive Cbl and folic acid supplements daily had Hcy plasma levels 30% lower than those given a placebo. For patients with Hcy levels in the top quartile, vitamin therapy correlated significantly with improvement in global cognition, episodic memory, and semantic memory, and the authors concluded that these B vitamins “appear to slow cognitive and clinical decline in people with mild cognitive impairment, in particular in those with elevated Hcy.”16
Despite the growing evidence supporting a correlation between Cbl and folic acid levels and neurological well-being, it is difficult to establish causation between low serum Cbl or low folic acid levels and conditions such as dementia, cognitive decline, and depression because these conditions may cause changes in appetite that may compromise nutritional intake.17 Dementia and depression may coexist among elders18; thus, it is important to explore the causal or permissive roles of insufficient or deficient serum levels of Cbl in the etiology of psychiatric disorders.
Based on data suggesting that folic acid and Cbl may have a role in preventing mood disorders and dementias, including Alzheimer’s disease and vascular dementia,8 current guidelines recommend checking Cbl levels in patients with cognitive impairment or as part of a dementia evaluation. If diagnosis and treatment of Cbl deficiency occur early in the course of cognitive decline, neuropsychiatric symptoms may be prevented or reversed,16 depending on their severity, the patient’s comorbid conditions, and the adequacy of treatment.
Cbl and the Cardiovascular System
Evidence supports a role for folic acid and vitamin B12 supplementation in lowering Hcy levels,19 but results from several large prospective studies do not show that supplementation decreases the risk of cardiovascular disease. The HOPE 2 (Heart Outcomes Prevention Evaluation 2) trial randomly assigned patients 55 years and older with vascular disease to a daily combination pill that included 2.5 mg of folic acid, 50 mg of vitamin B6, and 1 mg of vitamin B12, or to placebo. At a median of 5 years’ follow-up, Hcy levels in the vitamin B arm had declined an average of 2.4 µmol/L from baseline versus an average increase of 0.8 µmol/L in the control group. No statistically significant difference was observed between the groups in the mortality rate from cardiovascular events or myocardial infarction. Although patients taking placebo were more likely to have a stroke than patients receiving vitamin therapy (5.3% vs 4.0%; P=.03),19 when each of the primary outcomes was analyzed separately, there were no significant differences between groups in the rate of death from cardiovascular causes or myocardial infarction. Despite the risk of stroke being lower in the treatment group, the authors cautioned that the total number of events was low and the confidence interval wide, and the results were not adjusted for multiple comparisons. Because this was the only cardiovascular benefit observed with vitamin B therapy, the authors cautioned that the difference in stroke outcome might result from an overestimate or chance. An adjusted analysis showed an 11% decrease in the risk of coronary artery disease and a 19% decrease in stroke risk for patients whose Hcy levels dropped by 25%, suggesting a possible small benefit with vitamin B supplementation, but the authors said they were not confident enough in the finding to recommend vitamin B supplementation to prevent cardiovascular events.19
Skeletal Health
Cbl has been associated with osteoblast activity and bone formation,20-22 and a limited number of cross-sectional studies have associated low serum Cbl levels with decreased levels of markers of bone formation, such as serum alkaline phosphatase and osteocalcin.20,21 Epidemiologic evidence indicates a link between low serum Cbl levels and increased bone loss among older women.23,24
An analysis of data for the Framingham Offspring Cohort (n=2576) from the Framingham Osteoporosis Study found that men and women (80% postmenopausal) with a serum vitamin B12 level <148 pmol/L had significantly lower overall bone mineral density (BMD) and significantly reduced BMD in the hip and spine compared with those having higher serum B12 levels.23 A smaller study involving community-dwelling white women 65 years and older (n=83) enrolled in the Study of Osteoporotic Fractures found that those with a serum vitamin B12 level ≤207 pmol/L experienced an average annual decrease in hip bone density of 1.6% versus 0.2% annually for women with levels >207 pmol/L.24 Based on these findings, it is possible that ensuring elderly patients maintain optimal Cbl status will help preserve skeletal health.
Cbl Absorption and Transport
The RDA of vitamin B12 (2.4 µg/day)2 can be obtained by consuming one 3-oz serving of meat or fortified cereal daily. An estimated 50% to 90% of Cbl is stored in the liver, and the average adult liver retains an estimated 3 mg, with total body stores estimated to be up to 10 mg. These are relatively large stores, and in healthy adults who stop eating foods containing vitamin B12 (eg, such as those following a vegan diet) or who have subnormal Cbl intake, it may take 5 to 10 years to deplete existing stores and develop clinical manifestations of Cbl deficiency.25
Although the typical American diet contains a sufficient amount of Cbl to maintain normal levels, the complexities of Cbl absorption put even those with adequate intake at risk of deficiency. The digestive process for Cbl involves several steps taking place at various sites along the gastrointestinal tract. A defect compromising any step may induce Cbl insufficiency or deficiency.
Absorption of Cbl starts in the mouth, with small amounts absorbed from dietary sources via the oral mucosa; environments that are too alkaline, perhaps due to antacid use, thwart effective absorption.26 When the animal proteins to which the Cbl is bound arrive in the stomach, gastric acid and proteases cleave Cbl from the dietary protein to make it available for absorption.27 Free Cbl molecules bind to salivary haptocorrin (formerly called R binder), forming a Cbl-haptocorrin complex. This complex travels to the duodenum, where pancreatic enzymes lyse the Cbl-haptocorrin complex. The Cbl then binds to intrinsic factor (IF), which is secreted by gastric parietal cells.27 Cbl absorption takes place in the terminal ileum, where IF is removed from the complex and the vitamin is subsequently bound to transport proteins and delivered via the portal blood stream to the liver and other tissues.27 Free Cbl then attaches to transcobalamin (TC)-II, another carrier protein, and is released into the blood stream. Cbl attached to TC-II is referred to as holoTC-II and is taken up by liver, bone marrow, and other cells. Besides TC-II, vitamin B12 may also bind to TC-I and TC-III in human serum. All TC proteins are referred to as haptocorrins, and they are thought to serve mainly as transporters to the cell and to facilitate storage within the cell.28
Digestive Malabsorption
Cbl-food malabsorption is considered the most common etiology of Cbl insufficiency and deficiency among older adults and caused 60% to 70% of cases in one study involving 200 patients.29 Geriatric patients who develop chronic atrophic gastritis are at particular risk of impaired Cbl absorption due to reduced parietal cell secretion of IF and gastric acid.25 Although the patient is able to absorb free Cbl, the food-bound Cbl/protein complexes fail to separate and malabsorption results. Cbl-food malabsorption can also be caused by type B atrophic gastritis associated with Helicobacter pylori infections. In industrialized countries, nearly half of individuals 60 years and older are infected with H. pylori.3
Malabsorption resulting from small intestinal bacterial overgrowth (SIBO) is another important cause of Cbl deficiency in geriatric patients. It is thought that the uptake of Cbl by microorganisms in the small intestine may contribute to SIBO-related Cbl deficiency. Older adults have a higher prevalence of conditions that predispose them to SIBO, including reduced intestinal motility and achlorhydria.
Miscellaneous causes of vitamin B12 deficiency include gastric or intestinal resection, ileocecal tuberculosis, inflammatory bowel disease (Crohn’s disease), Whipple’s disease, tropical sprue, chronic pancreatitis, intestinal amyloidosis, primary gastric lymphoma, multiple myeloma, and human immunodeficiency virus. Rare genetic conditions, including TC deficiency, can also cause Cbl deficiency.28
Interactions With Pharmacologic and Biologic Agents
Nutrient–drug interactions can also lead to Cbl malabsorption or metabolic inactivation and should be a consideration for older adults, who are often taking multiple medications (Table26,30-35). Metformin, antibiotics, colchicine, and anticonvulsants are all known to contribute to Cbl malabsorption. Vitamin C, often prescribed to promote wound healing in elders, may contribute to the conversion of a proportion of dietary Cbl into a metabolically inactive analogue.35 Nitric oxide and other nitrates may also induce deficiency by oxidizing Cbl, particularly following anesthesia.36
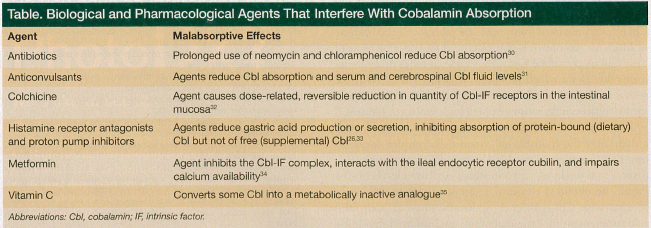
Gastroesophageal reflux disease (GERD) and acid reflux are common among older adults, and acid-lowering agents—prescribed and over-the-counter preparations—are among the most widely used medications. Their long-term use predisposes older adults to hypochlorhydria and SIBO, both risk factors for Cbl deficiency.37 GERD is often treated with proton pump inhibitors, which decrease gastric secretions. With prolonged use, proton pump inhibitors have been shown to inhibit Cbl absorption by as much as 70%3 and to significantly reduce serum Cbl levels.33
Metformin is often used to treat type 2 diabetes mellitus and metabolic syndrome, and Cbl malabsorption is a known adverse effect of prolonged metformin use. Approximately 20% of metformin users have low serum Cbl levels,34,38 and deficiency may occur as quickly as 3 months after initiating metformin.39 Megaloblastic anemia, hyperhomocyteinemia-induced deep vein thrombosis, and peripheral neuropathy have been reported in association with metformin-induced Cbl deficiency.40,41 Metformin-induced Cbl deficiency can also result in subacute combined degeneration of the spinal cord, which is easily mistaken for diabetic neuropathy.42 The scientific community has not reached a consensus regarding the mechanism of metformin-Cbl interaction. It has been suggested that several mechanisms may be involved, including inhibition of the Cbl-IF complex, interaction with the ileal endocytic receptor cubilin, and impaired calcium availability.24 Cbl-IF complex uptake by the ileal cell receptors is calcium dependent, and it has been suggested that metformin-induced Cbl deficiency may result from altered metabolism of intestinal calcium.
Assessing and Managing Cbl Levels in the Geriatric Patient
Although common and easily treated, Cbl deficiency and insufficiency are often under-recognized in older adults. Up to 20% of older Americans have marginal Cbl status, which can occur even when dietary intake appears to be adequate. In addition, Cbl levels considered normal have been observed in patients with clinical features of vitamin B12 deficiency.43-45 Because B12 and folate deficiencies may coexist, physicians should assess plasma Cbl and folic acid levels among all individuals 50 years and older, especially those with chronic conditions or who use medications known to limit Cbl absorption or gastric acid production (Table).
Total Cbl assay is usually the first test of choice for assessing Cbl status. Plasma levels of Cbl between 400 pmol/L and 500 pmol/L are currently thought to represent minimal optimum plasma Cbl levels for most elderly patients.46 Early depletion of Cbl is marked by low plasma levels of serum holoTC-II, and can be detected even when serum levels of total Cbl are normal. Serum holoTC reflects the fraction of vitamin B12 that is bound to circulating TC and is a sensitive marker of vitamin B12 status.47 A radioimmunoassay for the direct measurement of holoTC has recently become commercially available.48 Serum folate levels vary and are primarily a reflection of short-term folate balance rather than of tissue folate levels. For example, serum levels are higher following a meal that is rich in folate, but may be low following a few days of a dietary intake poor in folate. It is generally recommended that serum folate levels be obtained as an initial test, followed by obtaining red blood cell folate levels in those with a serum folate level <4 ng/dL.49
Before initiating metformin or other medications that can impair Cbl absorption or metabolism, Cbl and folate levels should be obtained. Among chronic users of metformin and other medications known to interfere with Cbl absorption or metabolism, Cbl levels should be maintained in the mid-normal range—at least 400 pmol/L to 500 pmol/L—and reassessed annually.
Treating Cbl Deficiency
Clinicians who treat older adults should seek to ensure that their patients maintain optimum Cbl status. Early recognition and repletion of suboptimal Cbl levels can help prevent illnesses and decreased quality of life associated with Cbl deficiency. Although Cbl is readily obtained from meats and other foods, the Institute of Medicine recommends that elderly adults consume most of their Cbl in crystalline form from fortified foods and supplements due to their high prevalence of achlorhydria.2 Whereas several analogues of Cbl exist, only adenosylcobalamin and methylcobalamin demonstrate physiologic activity in humans.50
If necessary, supplementation should be initiated with a daily over-the-counter oral vitamin B complex formulation that provides at least 100% of the RDA of vitamin B12. After 4 to 6 weeks of supplementation, plasma levels of Cbl should be obtained to assess response. If folate deficiency coexists with Cbl deficiency or insufficiency, an oral folic acid supplement of 1 mg daily for 1 to 2 months should be adequate. Once Cbl and folate levels have been repleted, an over-the-counter vitamin B complex formulation that provides 100% of the RDA of vitamin B12 and folate should be continued to maintain levels in the mid-normal range. We do not advocate folate intake >1 mg daily due to the potentially increased risk of colorectal and other cancers associated with folate supplementation at this level.51
In patients who fail to respond to oral Cbl therapy, nasal preparations of vitamin B12 can be administered at doses of 100 µg daily or 500 µg weekly. If response to oral and nasal therapy is insufficient, intramuscular treatment with 30 µg daily for 5 to 10 days followed by a 100 µg injection monthly should be initiated.
Conclusion
Vitamin B12, one of the most complex vitamins in nature, plays an important role in various essential functions of the body. The prevalence and impact of vitamin B12 deficiency is age-dependent, with older adults being the most susceptible, especially those who take multiple medications or have gastrointestinal problems. Cbl deficiency in elders is under-recognized in daily clinical practice, yet it can lead to irreversible neurological damage and increases a patient’s risk of osteoporosis and hematological diseases. Early detection and correction of Cbl deficiency are important steps in reducing the risk of these complications.
Drs. Ionica, Sourwine, and Steinle are from the Department of Medicine, University of Maryland School of Medicine, Baltimore; and Dr. Rochester is from the Department of Pharmacy Practice, University of Maryland School of Pharmacy, Baltimore. Dr. Steinle is also from the Baltimore Veterans Administration Medical Center, Baltimore, MD.
Dr. Steinle has received salary support in part from the Mid-Atlantic Nutrition Obesity Research Center (NORC), University of Maryland School of Medicine - NIH Grant P30 DK072488. The other authors report no relevant financial relationships.
References
1. Allen LH. USDA, ARS Western Human Nutrition Research Center. Bioavailability of vitamin B12. Int J Vitam Nutr Res. 2010;80(4-5):330-335.
2. Institute of Medicine. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academy Press, 1998.
3. Allen LH. How common is vitamin B-12 deficiency? Am J Clin Nutr. 2009;89(suppl):693S-696S.
4. Lindenbaum J, Rosenberg IH, Wilson PWF, Stabler SP, Allen RH. Prevalence of cobalamin deficiency in the Framingham elderly population. Am J Clin Nutr. 1994;60(1):2-11.
5. Centers for Disease Control and Prevention. Managing patients with evidence of a vitamin B12 deficiency. www.cdc.gov/ncbddd/b12/patients.html. Updated June 29, 2009. Accessed November 27, 2011.
6. Minot GR, Murphy WP. Treatment of pernicious anemia by a special diet—1926. Yale J Biol Med. 2001;74(5):341-353.
7. Ahrens RA. Mary Shaw Shorb (1907-1990) [published correction appears in J Nutr. 1993;123(8):1460]. J Nutr. 1993;123(5):793-796.
8. Miller AL. The methionine-homocysteine cycle and its effects on cognitive diseases. Altern Med Rev. 2003;8(1):7-19.
9. Selhub J, Troen A, Rosenberg IH. B vitamins and the aging brain. Nutr Rev. 2011;68(Suppl 2):S112-S118.
10. Reynolds E. Vitamin B12, folic acid, and the nervous system. Lancet Neurol. 2006;5(11):949-960.
11. Morris MS, Jacques PF, Rosenberg IH, Selhub J. Folate and vitamin B-12 status in relation to anemia, macrocytosis, and cognitive impairment in older Americans in the age of folic acid fortification. Am J Clin Nutr. 2007;85(1):193-200.
12. Hassan A, Hunt BJ, O’Sullivan M, et al. Homocysteine is a risk factor for cerebral small vessel disease, acting via endothelial dysfunction. Brain. 2004;127(Pt 1):212-219.
13. Werder SF. Cobalamin deficiency, hyperhomocysteinemia, and dementia. Neuropsychiatr Dis Treat. 2010;6:159-195.
14. Tangney CC, Aggarwal NT, Li H, Wilson RS, Decarli C, et al. Vitamin B12, cognition, and brain MRI measures: a cross-sectional examination. Neurology. 2011;77(13):1276-1282.
15. Lindenbaum J, Healton EB, Savage DG, et al. Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. N Engl J Med. 1988;318(26):1720-1728.
16. de Jager CA, Oulhaj A, Jacoby R, Refsum H, Smith D. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: a randomized controlled trial [published online ahead of print July 21, 2011]. Int J Geriatr Psychiatry. 2011. doi:10.1002/gps.2758.
17. Engel JH, Siewerdt F, Jackson R, Akobundu U, Wait C, Sahyoun N. Hardiness, depression, and emotional well-being and their association with appetite in older adults. J Am Geriatr Soc. 2011;59(3):482-487.
18. Vinkers DJ, Gussekloo J, Stek ML, Westendorp RG, van der Mast RC. Temporal relation between depression and cognitive impairment in old age: prospective population based study. BMJ. 2004;329(7471):881.
19. Lonn E, Yusuf S, Arnold MJ, et al; Heart Outcomes Prevention Evaluation (HOPE) 2 Investigators. Homocysteine lowering with folic acid and B vitamins in vascular disease [published correction appears in N Engl J Med. 2006;355(7):746]. N Engl J Med. 2006;354(15):1567-1577.
20. Van Dommelen CK, Klaassen CH. Cyanocobalamin-dependent depression of the serum alkaline phosphatase level in patients with pernicious anemia. N Engl J Med. 1964;271:541-544.
21. Carmel R, Lau KH, Baylink DJ, Saxena S, Singer FR. Cobalamin and osteoblast-specific proteins. N Engl J Med. 1988;319(2):70-75.
22. Eastell R, Vieira NE, Yergey AL, et al. Pernicious anaemia as a risk factor for osteoporosis. Clin Sci (Lond). 1992;82(6):681-685.
23. Tucker KL, Hannan MT, Qiao N, et al. Low plasma vitamin B12 is associated with lower BMD: the Framingham Osteoporosis Study. J Bone Miner Res. 2005;20(1):152-158.
24. Stone KL, Bauer DC, Sellmeyer D, Cummings SR. Low serum vitamin B-12 levels are associated with increased hip bone loss in older women: a prospective study. J Clin Endocrinol Metab. 2004;89(3):1217-1221.
25. Sethi N, Robilotti E, Sadan Y. Neurological manifestations of vitamin B-12 deficiency. The Internet Journal of Nutrition and Wellness. 2005;2(1).
26. Marcuard SP, Albernaz L, Khazanie PG. Omeprazole therapy causes malabsorption of cyanocobalamin (vitamin B12). Ann Intern Med. 1994;120(3):211-215.
27. Quadros EV. Advances in the understanding of cobalamin assimilation and metabolism. Br J Haematol. 2010;148(2):195-204.
28. Dharmarajan TS, Adiga GU, Norkus EP. Vitamin B12 deficiency. Recognizing subtle symptoms in older adults. Geriatrics. 2003;58(3):30-34,37-38.
29. Andrès E, Goichot B, Schlienger JL. Food cobalamin malabsorption: a usual cause of vitamin B12 deficiency. Arch Intern Med. 2000;160(13):2061-2062.
30. Cocke JG Jr. Chloramphenicol optic neuritis. Apparent protective effects of very high daily doses of pyridoxine and cyanocobalamin. Am J Dis Child. 1967;114(4):424-426.
31. Frenkel EP, McCall MS, Sheehan RG. Cerebrospinal fluid folate and vitamin B12 in anticonvulsant-induced megaloblastosis. Ann Gen Psych. 2008;7(suppl 1):S311.
32. Palopoli JJ, Waxman J. Colchicine neuropathy or vitamin B12 deficiency neuropathy? N Engl J Med. 1987;317(20):1290-1291.
33. Valuck RJ, Ruscin JM. A case-control study on adverse effects: H2 blocker or proton pump inhibitor use and risk of vitamin B12 deficiency in older adults. J Clin Epidemiol. 2004;57(4):422-428.
34. Andrès E, Noel E, Goichot B. Metformin-associated vitamin B12 deficiency. Arch Intern Med. 2002;162(19):2251-2252.
35. Hogenkamp HP. The interaction between vitamin B12 and vitamin C. Am J Clin Nutr. 1980;33(1):1-3.
36. Kinsella LJ, Green R. ‘Anesthesia paresthetica’: nitrous oxide-induced cobalamin deficiency. Neurology. 1995;45(8):1608-1610.
37. Schade SG, Cohen RJ, Conrad ME. Effect of hydrochloric acid on iron absorption. N Engl J Med. 1968;279(13):672-674.
38. de Jager J, Kooy A, Lehert P, et al. Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomised placebo controlled trial. BMJ. 2010;340:c2181. doi:10.1136/bmj.c2181.
39. Frayn KN, Adnitt PI, Turner P. The hypoglycaemic action of metformin. Postgrad Med J. 1971;47(554):777-780.
40. Köktürk N, Kanbay A, Aydoğdu M, Özyılmaz E, Bukan N, Ekim N. Hyperhomocysteinemia prevalence among patients with venous thromboembolism. Clin Appl Thromb Hemost. 2010;17(5):487-493.
41. Bell DS. Metformin-induced vitamin B12 deficiency presenting as a peripheral neuropathy. South Med J. 2010;103(3):265-267.
42. Tomkin GH, Hadden DR, Weaver JA, Montgomery DA. Vitamin-B12 status of patients on long-term metformin therapy. Br Med J. 1971;2(5763):685-687.
43. Wickramasinghe SN, Fida S. Correlations between holo-transcobalamin II, holo-haptocorrin, and total B12 in serum samples from healthy subjects and patients. J Clin Pathol. 1993;46(6):537-539.
44. Vu T, Amin J, Ramos M, Flener V, Vanyo L, Tisman G. New assay for the rapid determination of plasma holotranscobalamin II levels: preliminary evaluation in cancer patients. Am J Hematol. 1993;42(2):202-211.
45. Herbert V, Fong W, Gulle V, Stopler T. Low holo-transcobalamin II is the earliest serum marker for subnormal vitamin B-12 (cobalamin) absorption in patients with AIDS. Am J Hematol. 1990;34(2):132-139.
46. Allen LH, Casterline J. Vitamin B12 deficiency in elderly individuals: diagnosis and requirements. Am J Clin Nutr. 1994;60(1):12-14.
47. Hoey L, Strain JJ, McNulty H. Studies of biomarker responses to intervention with vitamin B-12: a systematic review of randomized controlled trials. Am J Clin Nutr. 2009;89(6):S1981-S1996.
48. Ulleland M, Eilertsen I, Quadros EV, et al. Direct assay for cobalamin bound to transcobalamin (holo-transcobalamin) in serum. Clin Chem. 2002;48(3):526-532.
49. Antony AC. Megaloblastic anemias. In: Hoffman R, Benz EJ, Shattil SJ, et al, eds. Hematology: Basic Principles and Practice. 4th ed. New York, NY: Churchill Livingstone; 2005:519.
50. Weinberg JB, Chen Y, Jiang N, Beasley BE, Salerno JC, Ghosh DK. Inhibition of nitric oxide synthase by cobalamins and cobinamides [published correction appears in Free Radic Biol Med. 2011;51(7):1471]. Free Radic Biol Med. 2009;46(12):1626-1632.
51. Cole BF, Baron JA, Sandler RS, et al, Polyp Prevention Study Group. Folic acid for the prevention of colorectal adenomas: a randomized clinical trial. JAMA. 2007;297(21):2351-2359.