
What is the cause of these cardiac abnormalities?
 THE CASE: A 13-year-old girl is admitted to the inpatient cardiology unit because of progressive dyspnea. She has a history of shortness of breath off and on for the past 2 months, and her symptoms are worse on the day of admission. She reports having general malaise, insomnia, a 10-kg weight loss, and amenorrhea for the past 4 months. She has no known drug allergies; her immunizations are up-to-date.
THE CASE: A 13-year-old girl is admitted to the inpatient cardiology unit because of progressive dyspnea. She has a history of shortness of breath off and on for the past 2 months, and her symptoms are worse on the day of admission. She reports having general malaise, insomnia, a 10-kg weight loss, and amenorrhea for the past 4 months. She has no known drug allergies; her immunizations are up-to-date.
On examination, the patient appears anxious. Ear, eye, nose, and throat findings are unremarkable. Chest expansion is symmetrical, with clear breathing sounds. Heart rate is 150 beats per minute. A grade 3 to 4/6 systolic murmur is audible over the left sternal border fourth to fifth intercostal space. Her extremities are freely movable without edema.
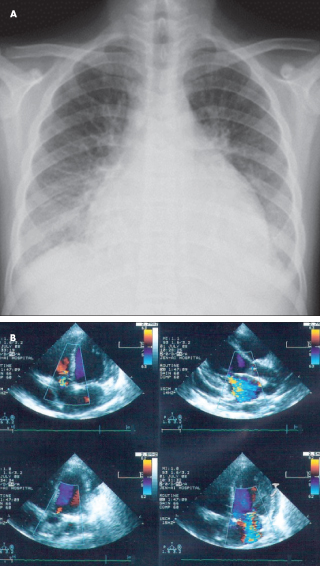
An ECG shows sinus tachycardia, with a heart rate of 130 beats per minute. A chest film on admission reveals cardiomegaly with pericardial effusion (A). Echocardiography confirms the cardiomegaly with compromised systolic function (left ventricular ejection fraction of 43.4%), massive pericardial effusion (greater than 10 mm), and moderate to severe mitral regurgitation with pulmonary hypertension (37.9 mm Hg) (B). The patient is treated with high-dose intravenous corticosteroids; however, her symptoms progressively worsen.
What might be the cause of the cardiac abnormalities in this patient?
- Myocarditis
- Cardiopulmonary or metastatic malignancy
- Autoimmune disease
- Metabolic disorder
Answer to Last Month’s Online Challenge
What might be the cause of the cardiac manifestations in this patient?
•Myocarditis
•Cardiopulmonary or metastatic malignancy
•Autoimmune disease
•Metabolic disorder
The correct answer is Autoimmune disease
An immunologist was consulted because of concern for systemic lupus erythematosus (SLE)-related cardiac abnormalities. Results of serologic tests for SLE were positive.
For the full case report and discussion, see “Pericardial Effusion With Heart Failure: Initial Sign of SLE in a Teenage Girl” in the March 2012 issue of Consultant For Pediatricians.