
PATIENT PROFILE:
After a long morning in the office, you finally pick up the chart for your last scheduled patient--17-year-old Michelle. Flipping through her chart, you remember seeing Michelle a few times last year for acne but otherwise her medical history is unremarkable. The chief complaint (documented by your triage nurse) is "headaches."
You enter the room and are greeted by Michelle and her mother. The mother seems anxious and begins by stating, "Michelle has been having headaches almost every day for the last 3 weeks. I'm sure she has a brain tumor."
Michelle concurs that she has been having almost daily headaches. These are fairly constant throughout the day and are described as a "mixture of pounding and squeezing." The pain is localized to the temples bilaterally and radiates to the occipital areas; it does not radiate down the neck or involve the upper or lower extremities. There is no diurnal variation to the pain, but it occasionally keeps her up at night.
Michelle insists that everything is fine at school and at home, and she denies any major life stresses. Her appetite has slightly decreased over the last few weeks because she has not felt well.
She denies any fevers, nausea or vomiting, photophobia, and phonophobia. Neither Michelle nor her mother remembers any recent trauma to the head. Michelle reports that her vision has "gotten worse"; however, a quick glance at your nurse's triage sheet reveals that the patient's vision is 20/20 in both eyes.
Michelle has been taking ibuprofen(, 400 mg bid for the past 3 weeks, with minimal success. Her only other medications are doxycycline( (for acne), which she takes daily, and topical tretinoin(, which she uses on her face.
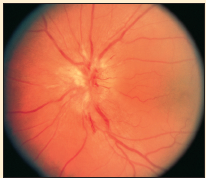 The physical examination reveals a young woman who appears somewhat uncomfortable but is in no acute distress. Results of examination of the HEENT, cardiovascular, and GI systems seem unremarkable. A funduscopic view is shown in the Figure. The neurologic examination reveals intact cranial nerves; reflexes are 2+ at the patellar, triceps, and biceps sites. Strength and sensation are both 5/5 bilaterally. The patient's gait is intact, and her coordination appears normal.
The physical examination reveals a young woman who appears somewhat uncomfortable but is in no acute distress. Results of examination of the HEENT, cardiovascular, and GI systems seem unremarkable. A funduscopic view is shown in the Figure. The neurologic examination reveals intact cranial nerves; reflexes are 2+ at the patellar, triceps, and biceps sites. Strength and sensation are both 5/5 bilaterally. The patient's gait is intact, and her coordination appears normal.
You ask Michelle to stare at your nose while you extend your hands to your sides and then ask her to tell you when she can see your fingers waving out of the corners of her eyes. You bring your hands in toward midline of the visual field and notice that she does not seem to see your finger movements until they are well within the center of the field.
WHAT WOULD YOU DO NOW?
A. Obtain a head CT scan today to rule out a brain tumor or other intra-cranial process.
B. Increase the ibuprofen dose to 800 mg and have the patient take it every eight hours for 3 days.
C. Recommend relaxation exercises and psychotherapeutic counseling for adolescent stress management.
D. Refer to the paient to a neurologist for further consultation.
Answer and discussion on next page
THE CONSULTANT'S CHOICE
The correct answer is A. The funduscopic examination reveals papilledema--which usually suggests an increase in intra-cranial pressure. This is certainly pathologic, especially in a patient with neurologic complaints, such as headaches or visual changes. A head CT scan must be obtained to rule out a brain tumor, abscess, blood/fluid collection, or other disorder.
While a short course of high-dose NSAIDs (choice B) may be indicated in some patients with chronic headaches, this choice would be inappropriate when physical findings suggest the possibility of a malignant process. Although many chronic pain conditions in adolescence are psychosomatic, the presence of visual changes and papilledema strongly suggests an organic origin to the pain rather than a somatization disorder. Remember, too, increased intra-cranial pressure must be evaluated and treated emergently, regardless of the cause. A neurologic consultation may be appropriate--but only if the patient can be evaluated within a few hours. A few days' wait to see the neurologist risks continued development of a potentially pathologic disease process. If a quick referral cannot be guaranteed, then the diagnostic and therapeutic workup needs to be initiated with neurologic consultation later if appropriate.
You decide to send Michelle for an immediate CT scan of the head. An hour later, the radiologist calls you to say that the head CT scan is essentially normal. No space-occupying lesion is noted, and there is no evidence of ventricular compression. The radiologist suggests obtaining an MRI to better delineate the structures. There is an opening in the schedule for a head MRI scan that afternoon (miraculously), and Michelle goes for the scan. At around 4 pm, the neuroradiologist calls and confirms the findings from the head CT scan: no abnormality was noted.
WHAT WOULD YOU DO NOW?
A. Reasured by the normal brain scams and neurologic examination results, you send the patient home with follow-up next week with a nueurologist.
B. Preform a lumbar puncture in the emergency department.
C. Refer the patient foe an ophthalmologic evaluation of the retinal findings that suggest papilledema.
D. Write a prescription for gabapentin( to treat a possible developing chronic pain syndrome (something you have seen in a number od adolescent patients).
THE CONSULTANT'S CHOICE
Somewhere in the back of your mind, you remember discussing "benign intra-cranial hypertension" during your intern year on the medical floor. You quickly do an online search and realize that you must send Michelle for a lumbar puncture performed with opening pressure measurements. Therefore, choice B is the correct answer.
At 10 o'clock that night, the emergency department physician calls you to report that Michelle's opening pressure was 257 mm H2O (normal is 10 to 20 mm H2O)and that she is feeling somewhat better after the procedure. The physician compliments you on your clinical acumen and comments that, while some practitioners might be complacent with the normal head scans, it is important to remember that neurologic complaints (such as headaches or visual changes) accompanied by retinal papilledema must always be considered an emergent situation that requires immediate evaluation and intervention (hence, choices A, C, and D are incorrect).
Michelle is admitted to the neurosurgery service with consultation from ophthalmology. Her admission and discharge diagnosis is pseudotumor cerebri.
PSEUDOTUMOR CEREBRI
Pseudotumor cerebri (otherwise known as idiopathic intra-cranial hypertension) has historically been referred to as benign intra-cranial hypertension. As its name suggests, increased pressure within the cranial cavity develops in the absence of any known structural or functional changes. While the disease state may be unrelated to a malignant or oncologic process, the condition often results in lasting morbidity--and in reality, it is anything but benign. In fact, if left untreated it can lead to permanent blindness.
A true cause of pseudotumor cerebri is unknown. A number of hypotheses have been suggested since the disease was first described over 100 years ago. One school of thought is that the increased intra-cranial pressure is the result of dysregulation in cerebrospinal fluid (CSF) production. The theory suggests that potential abnormalities in neurotransmitter production or receptors lead to an increase in CSF production by the choroid plexus, which further augments the pressure surrounding the brain and its structures. Other suggested hypotheses postulate that obesity leads to increased abdominal pressure, which subsequently provides an increased pressure gradient in the inferior and superior venae cavae that the cerebral venous return must overcome.
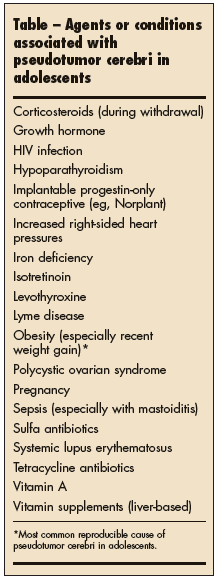 Epidemiologic data in children and adolescents are limited. Pseudotumor cerebri occurs in boys and girls with equal frequency during childhood. By late adolescence, girls are more often affected. The only truly reproducible risk factor for pseudotumor cerebri is obesity. That said, however, a number of agents or conditions are thought to contribute to the development of this disease state (Table).
Epidemiologic data in children and adolescents are limited. Pseudotumor cerebri occurs in boys and girls with equal frequency during childhood. By late adolescence, girls are more often affected. The only truly reproducible risk factor for pseudotumor cerebri is obesity. That said, however, a number of agents or conditions are thought to contribute to the development of this disease state (Table).
The "typical" patient with pseudotumor cerebri is an obese adolescent or young woman with some predisposing factor (a medication, for example, or a condition such as pregnancy). As described in this case history, the patient almost always complains of headaches that have been present for days to weeks. The head pain can occur in any location and may have almost any quality, but commonly it is described as a retro-orbital pain that worsens with eye movements.
Visual testing with Snellen charts can be normal, at least in the early stages of pseudotumor cerebri. However, if the condition is untreated, then tunnel vision, blurred vision, or total blindness can ensue. Visual complaints result from the increased pressure surrounding the optic nerves. (As mentioned in this case scenario, visual acuity was intact, but gross testing of peripheral visual fields was abnormal.) Some patients also complain of a constant pulsatile tinnitus consistent with blood flow through the high-pressure system inside the head.
Neurologic test results may be normal, although abducens nerve palsy has been reported. Funduscopic examination must be performed in any patient who complains of chronic headaches; the presence of retinal papilledema (often with the absence of retinal venous pulsations) should prompt urgent head imaging (via CT or MRI) to rule out an abscess or neoplastic process.
The imaging studies in pseudotumor cerebri are almost always normal, although they occasionally reveal small ventricles. If your patient has risk factors for venous thrombosis (such as smoking combined with oral contraceptive use), you might consider a venous angiogram or magnetic resonance venography to rule out a blood clot.
The lumbar puncture is both diagnostic and therapeutic for patients with pseudotumor cerebri. Opening CSF pressures should be measured. Typically, the obese adolescent with true pseudotumor cerebri has an opening pressure of 250 mm H2O. A thin adolescent who has an opening pressure of 200 mm H2O meets the criteria for this disease (levels below 200 mm H2O are suggestive but inconclusive for making the diagnosis). Results of CSF culture and cell counts are usually normal, although occasionally, protein levels may be increased.
Patients with pseudotumor cerebri should be managed in conjunction with an ophthalmologist and a neurologist (or neurosurgeon). The immediate goal is to decrease the intra-cranial pressure and alleviate obstructed blood flow to the optic nerves. This can be achieved through various modalities. Acetazolamide(, a carbonic anhydrase inhibitor, functions well as a diuretic; it has also been shown to decrease CSF production in the choroid plexus. Many neurologists recommend corticosteroids to decrease the intra-cranial pressure acutely, but they do not endorse the long-term use of these medications in the treatment of pseudotumor cerebri.
When vision appears markedly impaired, the ophthalmologist may perform a decompression procedure called an optic nerve fenestration in which small slits are made in the optic nerve sheath. This helps relieve the pressure on the optic nerve and allows for increased blood flow to the nerve. The procedure generally stabilizes or diminishes the visual deficits, although the extent of improvement varies between studies. Other modalities for preserving vision involve reduction of intra-cranial pressure through serial lumbar punctures or placement of a lumboperitoneal shunt for longer-term pressure reduction.
If one of your patients has pseudotumor cerebri, make sure to eliminate any predisposing factors. In the case of Michelle, she had been taking doxycycline for her acne. Although tetracyclines are commonly used to treat adolescent acne, it is quite possible that this agent contributed to the development of the disease. Topical vitamin A preparations (such as Michelle's tretinoin) have not been reported to cause pseudotumor cerebri, but any patient with pseudotumor cerebri should discontinue systemic vitamin A supplements (such as isotretinoin() as soon as possible. And, of course, long-term treatment involves an aggressive but healthful weight loss plan in the obese adolescent.