
 SANJAY KHUBCHANDANI, MD and VASUNDHARA TOLIA, MD Children’s Hospital of Michigan and Wayne State University
SANJAY KHUBCHANDANI, MD and VASUNDHARA TOLIA, MD Children’s Hospital of Michigan and Wayne State University
A 9-year-old girl was seen in the emergency department (ED) with a 5-day history of non-bilious, non-projectile emesis, decreased appetite, and persistent right lower quadrant pain following an appendectomy 5 days earlier. The appendectomy was performed after 2 days of abdominal pain and emesis. During the surgery, the appendix appeared normal. Surgeons noticed superior mesenteric lymphadenitis thought to be secondary to a viral illness. The patient was discharged home without any symptoms.
In the ED, the patient felt warm to the touch, but she had no history of chills or rigors. Her bowel movements were normal (1 or 2 daily), and she had no history of diarrhea or constipation. She had been able to tolerate oral intake until the day before her ED visit, after which she had 2 episodes of emesis. The patient had no history of recent travel, exposure to pets, documented fever, respiratory symptoms, sore throat, sick contacts, trauma, or urinary symptoms. She had not received any medications except for acetaminophen.Her mother had a history of kidney infection.
The patient was afebrile with stable vital signs. She had lower abdominal tenderness without guarding. She appeared uncomfortable, with tenderness and guarding at the surgical site and in the periumbilical region. She also had a fading erythematous rash on both cheeks. The surgical site was clean with no discharge. Rectal examination was normal, with no occult blood.
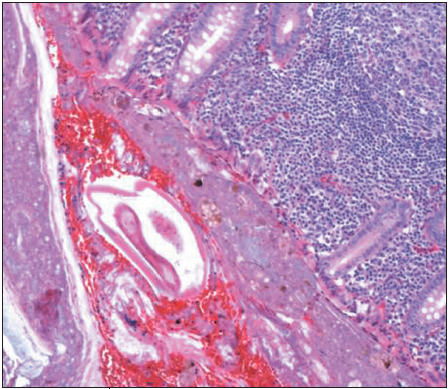
The patient's complete blood cell count was normal, as were levels of liver enzymes, amylase, lipase, elec- trolytes, blood urea( nitrogen, and creatinine. Abdom- inal radiographs were normal. Appendiceal biopsy specimen appears above. The patient was admitted for observation.
To what diagnosis do the clinical and histologic pictures point?

DISCUSSION
Pinworm infection--also known as seatworm or threadworm infection, enterobiasis, or oxyuriasis--is caused by intestinal infestation with the tiny 1-cm-long helminthic worm Enterobius vermicularis. Pinworm infection is the most common helminth infection worldwide.1 An estimated 200 million people are infected-- including about 40 million people in the United States and Canada.
Pinworms are usually harmless. Most commonly, they cause anal pruritus.1 However, serious complications--such as enterocutaneous fistulae,2 urinary tract infections,3 and salpingitis4--can occur. Schoolchildren are at highest risk for pinworm infections: this helminthic infestation has been reported in 0.2%5 to 2.4%6 of children presenting with apparent appendicitis. In appendiceal specimens removed because of symptoms of acute appendicitis, pinworms were found more frequently in girls (4.6%) than in boys (1.9%).7,8 A recent study showed that 1.4% of the appendiceal specimens removed for various diagnoses contained pinworms.8
Humans are the only biologic hosts of pinworms. Infestation begins when embryonated eggs (which are found under fingernails, in dust, and on clothing) are ingested. They hatch in the stomach into larvae, which travel to the cecum and ascending colon, where they mature into adult females (10 mm long) and males (3 mm long). Gravid females migrate by night to the perianal area, where they deposit their eggs; this gives rise to anal pruritus. Children reinfect themselves through scratching and dirty fingernails. Pinworm eggs, which are relatively resistant to desiccation, also contaminate clothing and bed linens--where they remain viable and infectious for 2 to 3 weeks.
Fecal sampling is rarely sensitive. The diagnosis is made at night or in the early morning with the application of cellophane tape to the child's perianal area.
The clinical picture of pinworm infection varies. At one end of the spectrum, parasites may be present in the appendiceal lumen without inflammation or mucosal penetration. At the other end is acute or chronic inflammation, obstruction, and appendicealrupture.
Treatment is relatively inexpensive and simple. A single dose of mebendazole( (200 mg) in children aged 2 years and older or a single dose ofpyrantel pamoate (11 mg/kg) in children 3 years and older is considered adequate treatment. A repeated dose 2 to 3 weeks later is recommended to target unhatched ova. Treatment of family members--particularly siblings--is also recommended. Immunity to pinworms does not develop in humans, and reinfection is therefore common.