
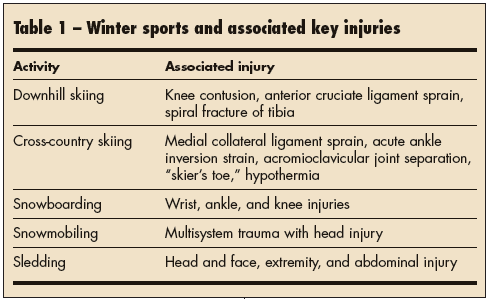
Millions enjoy skiing, snowboarding, and sledding. These cold weather activities--while exhilarating--also cause many injuries, each with distinct clinical characteristics (Table 1).
Here I discuss the injuries associated with skiing, snowboarding, snowmobiling, and sledding. The emphasis is on pediatric injury patterns and modes of treatment and prevention.
Alpine, or downhill, skiing is one of the world's most popular winter sports. However, it also carries a high risk of injury, the most common of which are:
• Knee contusion in children.
• A sprain of the ulnar collateral ligament of the thumb in adolescents.
• A grade 3 sprain of the anterior cruciate ligament in adults.
The use of properly functioning modern equipment can decrease the rate of skiing injuries, especially in children.
Most investigators agree that younger skiers are at increased risk. Children have a higher rate of ski-related fractures of the lower extremities than adults, for example. Spiral fracture of the tibia is most common in children.
Improperly adjusted or poor-quality bindings and boots may account for the higher rate of injury. Children often use outdated hand-me-down equipment that does not fit or function properly. It is important to educate parents about providing modern equipment and to verify that the binding settings function appropriately for the child using the equipment.1
In a 5-year retrospective study of patients younger than 19 years who were admitted to a pediatric trauma center after a skiing accident, 58% had been involved in collisions with stationary objects.2 Helmet use was negligible.
Between 20 and 30 deaths from downhill skiing accidents occur each year in this country. The cause of death is massive head or neck injury, and/or major thoracoabdominal injury. The main contributing factors are excessive speed and loss of control. Drugs and alcohol( are rarely implicated. One study found that only 1 in 16 injured skiers was wearing a helmet.3
Prevention efforts. Parents must not overestimate their child's skill level. Advise them to discourage skiing near the edge of trails. Adult supervision of children and adolescents is advised.
Oh and Schmid4 have gone so far as to recommend compulsory helmet use by all young recreational skiers. Theoretically, this is reasonable, but studies of helmet effectiveness have not been done. Design problems concerning sight and hearing still exist. Helmets tend to be costly and, because they must fit closely, must be purchased frequently for growing children. In a review of winter sports injuries, knee sprain was the most common injury (in 31%); this was followed by general bruising (10%) and laceration of the head and face (8%).5
CROSS-COUNTRY SKIINGCross-country skiing offers excellent cardiovascular conditioning without the jarring and pivoting of many aerobic sports. It is generally affordable and accessible to both recreational and competitive enthusiasts. It is also relatively safe, although not risk-free. The rate of associated injuries is difficult to establish because recreational skiers ski wherever snow is available and not necessarily at ski areas that provide immediate medical assistance.
Backcountry skiing involves additional risks--avalanches and hypothermia among them. In general, the risk of injury decreases with increased experience and ability. However, injury patterns differ at different skill levels, and the average severity of injury may be higher among advanced skiers.
The lower extremity is at greatest risk and is affected in just over half of injuries. A sprain of the medial collateral ligament of the knee occurs after a valgus stress is applied to the knee, often when the skier catches a ski tip or edge while the leg is in a fixed position.
Ankle injuries. Theseare also common, particularly the acute inversion ankle sprain. Radiographs are needed to rule out ankle fracture in skiers who have bony tenderness directly over the lateral malleolus, the navicular, or the base of the fifth metatarsal; who have tenderness around the medial malleolus, the anterior ankle joint, and the syndesmosis; or who are simply unable to bear weight.
Acute, nonoperative treatment of ankle sprain involves rest, application of ice, compression, and elevation. Early range-of-motion exercises, such as tracing the alphabet with the great toe, and proprioceptive exercises done on a balance board or mini trampoline assist recovery. Sprains resulting from a significant rotatory force (eg, from a high-speed fall on downhill terrain) are often more severe, may take 6 weeks to improve, and may require more prolonged rehabilitation.
Shoulder injuries. Acromioclavicular joint separation, common among cross-country skiers, can occur when the skier falls directly on the shoulder. Pain is present directly over the acromioclavicular joint, and deformity is seen in grade 2 and 3 sprains. Treatment is usually nonoperative and includes early range-of-motion exercises followed by shoulder-strengthening exercises. Shoulder dislocations, rotator cuff tears, and fractures of the clavicle have also been reported.
Overuse injuries. Thesemost often result from training errors or errors in technique. Treatment is individualized but, in general, therapy involves relative rest, stretching and strengthening exercises, and a gradual return to skiing.
Cold- and wind-related injuries. Cross-country skiers are often out on open terrain with little protection from the wind. Their speed can worsen the wind's effect. In fact, a skier moving 30 km/h (20 mph) in calm air at 210°C (14°F) is exposed to a windchill of 225°C (213°F). Such temperatures can result in frostnip or frostbite.
Prevention. Attention to equipment is important for prevention of traumatic and overuse injuries. Boots, poles, and skis should be properly fitted to the skier and his or her skiing style to help minimize the potential for falls and overuse injuries. Properly waxed skis can prevent repeated backward slipping on icy, hard tracks, which can overstress muscle-tendon units.
Prevention strategies for overuse injuries focus on technique improvement, proper warm-up and cooldown exercises, and endurance and strengthening exercises for the muscle groups involved. Roller skiing as off-season training has increased in popularity and can be part of a good prevention strategy. Layered clothing, adequate hydration, and protective eyewear help prevent cold- and wind-related injuries.
SNOWBOARDINGSnowboarding is the fastest-growing winter sport in the United States. It involves riding a single epoxy-fiberglass board (resembling a large skateboard) down a ski slope or on a half-pipe snow ramp (a specialized snow structure used for performing tricks).
Snowboarding differs from downhill skiing in many respects. Snowboarders ride with both feet affixed by non-releasable bindings to a single board. Unlike downhill skiers, snowboarders stand perpendicular to the long axis of their boards. Furthermore, snowboarders do not use ski poles, but use their hands and arms for balance (much like skateboarders or surfers). Associated injuries frequently involve the upper extremities and ankles. The knees are less frequently involved than in traditional alpine skiing.6
Prevention. Wrist guards are very effective in preventing wrist injuries among in-line skaters and may also help prevent snowboarding injuries. Although protective equipment decreases the overall incidence of injury by reducing the force of impact, it may actually place the areas proximal to the device at increased risk by shifting the distribution of impact forces. For example, skiers and snowboarders who wear hard boots are at greater risk for "boot-top" fractures, and in-line skaters are at greater risk for "wristguard-top" fractures. This effect is illustrated in a survey that included 21 snowboarders who had been injured while wearing wrist guards: although none of these persons had a wrist injury, 6 had a shoulder injury and 4 had radial shaft fractures.7
Lower leg fracture was more than 3 times as common among injured children as among teenaged and adult alpine skiers. Dislocation increased with age for both alpine skiers and snowboarders. Injury severity seems to increase with age: more adults than children need to be treated by a physician or in a hospital for their injuries.8
Spinal injuries.These are among the most devastating injuries associated with all winter recreational sports. Tarazi and coworkers9 reported that the incidence of spinal injury among skiers was 0.01 per 1000 skier days and that among snowboarders it was 0.04 per 1000 snowboarder days.10 Jumping was the cause of injury in 20% of skiers and 77% of snowboarders. Neither age nor sex accounted for any significant portion of this difference. The rate of spinal injuries among snowboarders is 4-fold that of skiers.
SNOWMOBILINGWith vehicles that reach speeds of 90 mph and that weigh more than 600 lb, it is not surprising that snowmobiling culminates in more than 200 deaths and nearly 14,000 accidents each year.10,11
Pediatric injuries. Incredibly, children younger than 17 years sustain 12% of all snowmobile injuries. Pyper and Black12 reported 70 snowmobile-related injuries in persons aged 2 to 17 years. These injuries had been caused by losing control of the sled, rollover, striking a fixed object, or striking a motor vehicle or another sled. Fifteen accidents involved more than 1 person, and 5 of the injured children were pedestrians. Three deaths in this series were related to head trauma.
The Consumer Product Safety Commission's database on children and snowmobiles contains information on 291 injuries and 75 deaths for 1990 through 1998.13 The commission reported that many states have no age or helmet regulations regarding snowmobile use.
The American Academy of Pediatrics reviewed available snowmobile injury data from 1997 through 1998.14 During that time, there were more than 10,000 emergency department visits related to snowmobiling accidents. Ten percent of those involved were younger than 15 years. Head trauma was the leading cause of death.
SLEDDINGBecause it is a family affair, sledding often involves very small children--those at highest risk for head injuries. Children younger than 6 years had 3 times as many head injuries as those older than 12 years.15 There are several contributing factors. Children younger than 12 years have proportionately large heads, higher centers of gravity, and lower levels of coordination and muscle strength.
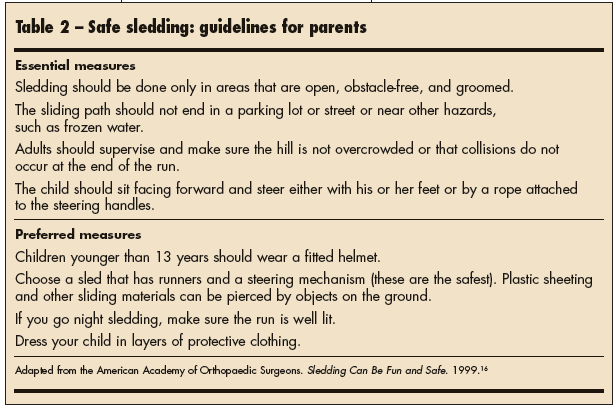
Spurred by the steady rate of sledding injuries and the rising interest in many forms of winter sliding activities, the American Academy of Orthopaedic Surgeons has published guidelines for safe sledding.16 These recommendations are divided into essential and preferred components and focus on the environment of the activity, the instruments of sledding, and the operator (Table 2).
In general, children are more likely to sustain upper extremity injuries than adolescents and adults. Children younger than 10 years incur more fractures and catastrophic injuries (head injuries) with individual recreational activities than they do during organized sports.17
Key preventive measures are available online at http://www.kidsource.com/safety/winter.sport.safety.html.18
For the patient with musculoskeletal injury, there are 4 phases of rehabilitation19:
1. Limiting additional injury; controlling pain and swelling.
2. Improving strength and flexibility of injured structures.
3. Progressive improvement in strength, flexibility, proprioception, and endurance of the injured structures until near-normal function is achieved.
4. Returning to the sport gradually through functional rehabilitation.