
What Do These Images Reveal?
Right ankle pain after a basketball injury
A 29-year-old man presents with right ankle pain caused by a basketball injury he sustained 1 day earlier. He fell after he had jumped up and landed on another player’s foot. The patient’s foot was “turned in” during the fall; this position indicates an inversion injury. He says he has injured his ankle before but never this severely. The rest of the medical history is noncontributory.
 |  |  |
| Top 10 Summer Sports With the Most Injuries | |
Sports | No. of injuries 1,633,905 1,498,252 492,832 477,647 406,381 246,875 233,806 196,260 189,942 187,391 |
| From the American Academy of Orthopedic Surgeons (2000). | |
You order conventional radiographs of the right ankle. What abnormalities are evident on these films and what further investigation is warranted?
(Answer on next page.)
Right ankle pain after a basketball injury: The frontal view of the ankle reveals soft tissue swelling that is predominantly lateral (A, yellow arrow). A small ossific fragment is evident distal to the lateral malleolus (A, white arrow); close inspection shows this to be well-corticated. The remainder of the osseous structures are intact. The lateral view reveals a joint effusion in the talotibial joint (B, arrow); no fractures are visible. In the oblique view (C), the osseous structures appear intact.
 |  |  |
The well-corticated ossific fragment is consistent with an old injury, but it is in the region that is now extremely tender. The joint effusion indicates that the current injury is severe. However, this is a nonspecific finding; joint effusions are seen with fractures and ligament and tendon injuries.
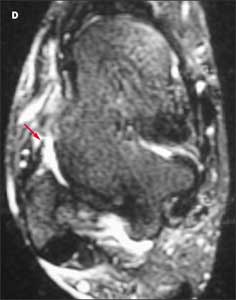
Because the patient’s pain is severe, you order an MRI scan to further evaluate the injury. A T2-weighted axial image reveals disruption of the anterior talofibular ligament (D, red arrow).
Ligamentous injuries are classified as follows:
•Grade 1: the ligament is overstretched but not actually torn; this is the most common and least severe type of injury.
•Grade 2: a partial tear without complete disruption of the ligament; this is a more serious injury.
•Grade 3: complete disruption of the ligament with subsequent instability.
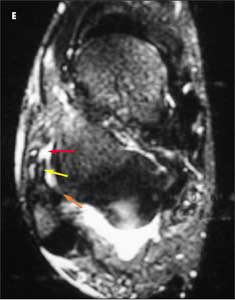
This patient has a grade 3 injury to the anterior talofibular ligament. In another axial T2-weighted image (E), fluid (yellow arrow) is visible in and around the course of the ligament (red arrow). This confirms that the disruption is acute. The posterior talofibular ligament appears normal and intact (E, orange arrow).
Patients with injuries of this ligament often do not seek medical attention, and it can be difficult to distinguish between acute and more remote injuries on imaging studies. Acute tenderness and fluid at the site of the disruption are 2 clues that can help identify an acute injury.
 |  |  |
A coronal T1-weighted image shows thickening of the calcaneofibular ligament (F, arrow); however, the fibers of the ligament are intact, which indicates that the injury is microscopic (a grade 1 injury). On all the images, the lateral malleolus is normal and intact, which rules out fracture.
The final diagnosis is acute complete disruption of the anterior talofibular ligament (grade 3 injury) with microscopic injury of the calcaneofibular ligament (grade 1 injury). This pattern is common in inversion injuries of the ankle. Typically, the ligaments of the lateral aspect of the ankle are injured in the following sequence:
•The anterior talofibular ligament, which resists the distracting forces created when the talus and fibula are inverted, is the first to be disrupted.
•The calcaneofibular ligament is the second ligament injured.
•The posterior talofibular ligament— if it is injured at all—is the third ligament injured.
Outcome of this case. The patient was immobilized for 6 weeks and the ligamentous injuries healed.